Kjetil Larsen, CES
Corrective Exercise Specialist, Training & Rehabilitation, Oslo (Norway)
Correspondence: Kjetil Larsen, CES, Corrective Exercise Specialist, Training & Rehabilitation, Oslo (Norway); Tel.: +47 975 45 192; E-mail: Kjetil@trainingandrehabilitation.com
ABSTRACT
A commonly used postural corrective measure is to pull the shoulders back and down. This corrective measure is most likely based upon the idea that postural acromial protraction is a frequent tendency in neck and shoulder patients, as is excessive clavicular elevation during shoulder movement. However, this corrective measure is based upon logical fallacies, firstly because it will cause scapular depression and downward rotation, which has been associated with scapular dyskinesis (SD), shoulder impingement syndrome (SIS) and neck pain. Secondly, biomechanically it will set the patient in the Halstead’s costoclavicular compression (“military brace”) test position, which may result in plexopathy and thoracic outlet syndrome (TOS). The corrective measure thus opposes what it is intended to do, as it may exacerbate neck and shoulder problems rather than ameliorating them. Based on the anatomy and evidence, as well as personal clinical experience with 115 TOS patients, it is my impression that the cue in question is harmful and that its use should be discontinued. Conversely, the patient should be cued to raise his or her scapulae until the superior scapular angles are levelled with the T2 vertebra, and learn to stay there, as this will upwardly rotate the scapulae as well as decompress the costoclavicular space.
Keywords: Thoracic outlet syndrome; Costoclavicular space syndrome; Scapular posture; Shoulder impingement syndrome; Scapular dyskinesis
Citation: Larsen K. Postural cues for scapular retraction and depression promote costoclavicular space compression and thoracic outlet syndrome. Anaesth Pain & Intensive Care 2018;22(2):256-267
Received – 28 June 2017, Reviewed – 29 June 2018, Corrected & Accepted 30 June 2018
INTRODUCTION
The notion that proper scapular posture involves pulling the shoulders “back and down” is widely accepted and practiced by several current musculoskeletal practices, as well as by exercise trainers.1-6 However, pulling the clavicle back and down may compress the costoclavicular space and cause thoracic outlet syndrome: In fact, the Halstead’s “military posture” stress test, a provocative test for costoclavicular space (CCS) compression, involves these exact clavicular movements.7-14 Intentional scapular depression also promotes downward rotation and anterior tilt, which has been associated with neck pain, scapular dyskinesis (SD), shoulder impingement syndrome (SIS),15–35 and neck pain.6,35-39 The aim of this article is to look at the origin of the “back and down” postural corrective measure, demonstrate its harmful implications, and to provide alternative criteria for assessment and correction.
The notion itself most likely originates from earlier studies, mainly those addressing SD and SIS where it was shown that patients with these afflictions tend to have an anteriorly situated clavicle/acromion in posture,31,34,40 implying scapular anterior tilt, downward rotation and protraction. Earlier studies have also shown that patients with SIS have a tendency of clavicular elevation as well as scapular downwards rotation and anterior tilt on the affected side during glenohumeral articulation.24-29,34-35 It has also been documented that patients with neck pain have a postural tendency of anteriorly positioned clavicles with downward scapular rotation.6,35-39 Some of these authors recommended postural correctives, which involved scapular retraction.40-43
Since the literature suggests that anterior drooping in posture, as well as anterior tilt and downward rotation during shoulder flexion and abduction, one could recommend some degree of scapular retraction as a corrective measure. However, stemming from the powerlifting and fitness communities,1-5 depression of the scapula was also included in this corrective strategy. As mentioned, scapular retraction and depression may promote CCS compression as well as SD with concomitant SIS. Therefore, it would seem that this corrective intervention is not based upon evidence nor sound biomechanics.
SCAPULAR RESTING POSTURE
Researchers have estimated that optimal longitudinal resting position of the scapula is when the superior scapular angle is levelled with the T2 spinous process, 0-5˚ of upwards rotation and approximately 20˚ of clavicular retraction and 20-25˚ of upwards clavicular inclination.6,10,11,14,16,34,44-48
By pulling the scapulae back and down, the only criteria that will be met as regards optimal position, will be retraction. It will also cause depression, anterior tilt (from squeezing the shoulders together,11 and downward rotation, which completely opposes the corrective’s original purpose i.e. to increase upwards rotation and posterior tilt, as well as retraction. Either way, this may cause continuous postural lengthening and inhibition of the trapezius and levator scapulae, often resulting in cervical stiffness,49 cervical myofascial tenderness and pain,6,15,37-39 scapular dyskinesis and shoulder impingement syndrome,6,24-29,34,35,40 and rotator cuff injuries.30,33
Although quite troublesome, shoulder and neck pain, etc. are still considered of lesser significance compared to costoclavicular compression syndrome, which normally involves compression of the brachial plexus, subclavian artery & subclavian vein between the clavicle and 1st rib, but may also occur against the 2nd rib.50 Retraction and depression of the scapulae may lead to osseous compression of the costoclavicular space,7-14 as it quite literally puts the patient’s clavicle in continuous Halstead’s costoclavicular compression test (“military brace”) position, often resulting in thoracic outlet syndrome (TOS).
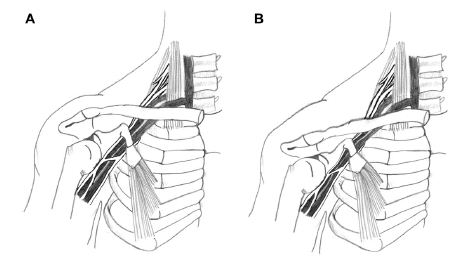
Figure 1: Costoclavicular space compression (Image source: Watson et al., 2010)
It is well documented that TOS patients tend to have depressed scapulae, along with anterior tilt,10-14,44-46,51-60 which further depresses the clavicle. Watson states that scapular depression along with dyskinesis is commonly seen in TOS patients, and that this encourages costoclavicular compression.11 Elevating the scapulae will decompress the CCS,58 which is also an orthopedic test called the Cyriax test.8 This is one major reason why TOS surgery involves resection of the 1st rib; to free the neurovascular bundle within the CCS. It is therefore of paramount importance to ensure that patients do not overly depress their scapulae, to avoid oblivious CCS compression. Figure 1 illustrates how depression and retraction of the clavicle may compress the neurovascular bundle. Contrarily, lifting the clavicle will decompress the neurovascular bundle.
COSTOCLAVICULAR SPACE COMPRESSION
Compression of the neurovascular bundle (NVB) of the thoracic outlet may lead to plexopathy, muscular atrophy,61-65 carpal tunnel syndrome (double crush),65-68 chest pain, ulnar neuropathy,65-72 dorsal scapular neuralgia73,74 arm swelling and cyanosis.75,76 Other symptoms are Raynaud’s syndrome,75,76 positional ischemia or venous insufficiency,69,72,77-80 which may contribute to intracranial hypertension83 and migraines in addition it may present as digital sensory loss 72), hand sweating and coldness.98–99,107–108 secondary dysautonomia such as atrial fibrillation and vasoconstriction.81,98–103 deep vein thrombosis (DVT) development,79,88-93 weakness of the extremities, chest pain and pseudoangina,69-71,88-90 subclavian artery injuries with subsequent embolus,73,96 which may lead to retrograde thromboembolism with sequelar stroke,91-93,97.98 and more.
Because of the vast spectrum of symptoms that may appear in the sequela of TOS development, TOS may reveal itself with any of the above-mentioned symptoms. It is well known that these symptoms are not unique,79,99 and it is hard to diagnose and treat the condition.78,100-104 This is one of the main reasons why (occult) TOS may be misdiagnosed as carpal tunnel syndrome, ulnar neuralgia, idiopathic chest pain, etc., in its beginning and intermediate stages. Neurographies (MR neurography imaging (MRN), electromyography (EMG), electroneurography (NCV), somatosensory evoked potentials (SEP) are insufficiently sensitive for detection of TOS, and may only be positive in very advanced stage.72,105-112 Rousseff et al.111 states that EMG / NCV is useless for identification of TOS, as 18 out of 20 patients with very obvious TOS symptoms had normal electrodiagnostic results. A systematic review conducted by Kwee et al.112 concludes that MRN is not sensitive nor specific enough for detection of brachial plexus neuropathies nor other peripheral neuropathies. This further complicates the likelihood of these patients (i.e. a victim of the “chronic Halstead’s maneuver”) to be properly diagnosed and treated.
It is a misfortune for patients to be iatrogenically set into the “back and down” scapular posture, as they may not be diagnosed until many years later due to the diffuse presentation of TOS.
CLINICAL PRACTICE & APPROPRIATE CORRECTIVES
In this section I will provide some criteria for identification of TOS as well as scapular resting dysfunction. Neurogenic TOS is the utmost common variant, which makes up approximately 95% of total TOS incidences.78,79,113 Because the inferior trunk lies more susceptibly (anteriorly) placed in the CCS, symptoms of C8-T1 (ulnar) neuropathy may appear first. However, the superior trunk (C7) and middle trunk (C5-6) may be affected, especially in more progressed cases of TOS.65,72 Supraclavicular tenderness (Morley’s test) and weakness of the 5th finger are sensitive, and relatively specific tests for thoracic outlet syndrome.69-71,78-79,99,100,113-116 Weakness of the triceps (C7 myotome) is also common. There may also be positional ischemia upon shoulder elevation, demonstrated by a white hand sign,69-71,116-119 indicating severe compression of the subclavian artery.59,88,116,120,121 One test alone, e.g. Adson’s or Roos’ test, may not be specific enough to diagnose TOS, especially because only 5% of TOS incidences are considered to be of vasculogenic dominance.
Compression of the CCS may occur related to posture or intermittently during certain activities. For example, a patient may have a seemingly normal scapular resting height, but still have a tendency of pulling their scapulae back and down during exercise, or have scapular dyskinesis, which may lead to intermittent compression of the neurovascular bundle. It is important to examine the patient’s scapular position as well as loaded and unloaded movement pattern in different scenarios. In addition Halstead’s CCS test may be used during the examination. A detailed explanation of identification and correction of scapular dyskinesis is outside the scope of this article.
The longitudinal scapular height can be measured by palpating the C7 (vertebra prominens) spinous process, then counting down to the T2 level, and comparing it to the level of the superior scapular angle. Up-/downwards rotation can be measured vertically by evaluating the angle of the medial scapular border, or horizontally, the angle of the scapular spine. The scapula is in downward rotation if the spine is pointing caudally, or if the superior angle is lateral to the inferior angle (sagittal axes). Anterior-/posterior tilting can be evaluated by measuring how far anterior the acromion is in relation to the inferior scapular angle, in the sagittal plane (coronal axis). An inclinometer, which in modern times is available for download on any smartphone, can also be used reliably to measure scapular angulation.11,23-26,40,122-128
The Cyriax release test is another orthopedic test which relieves the CCS by elevating the clavicle.8 Thus, postural CCS compression may be ameliorated by raising the shoulders slightly,58 and staying there .This will also upwardly rotate the scapula,55 which is important for SD and SIS treatment. To correct scapular slouching, ask the patient to lift their acromion until the clavicle is elevated and superior scapular angle is approximately levelled with the T2 vertebra, and the scapula is in mild upwards rotation. The patient must be educated with regards to the etiology of costoclavicular space compression syndrome, so that they become sufficiently motivated to maintain their newly acquired posture. Further, he or she must learn to maintain adequate scapular height during glenohumeral articulation.
Figure 2 shows a 25-year-old patient with chronic brachial, periscapular, chest and neck pain. She had been vigorously pulling her scapula back and down to “relax” her shoulder girdle, inevitably worsening the situation. Selmonosky’s DT was positive, as was Halstead’s CCS maneuver. Both scapulae were situated at the T4 vertebral level; very depressed (Figure 2, left). The left scapula was slightly more depressed than the right one and more caudally rotated as well. There was also bilateral scapular dyskinesia present during movement and loading of the arms. After identifying the scapular depression, the patient was cued to lift her acromion while slightly elevating the scapulae towards the back of the head, as to promote scapular elevation and upwards rotation with slight retraction, until the scapular angle was parallel with the T2 spinous process. She was told to stay there (Figure 3), and we also practiced moving and loading the arms while maintaining proper scapular height and angulation. The reason for cueing the patient specifically to lift the acromion rather than just the scapula, is that this promotes upwards rotation due to upper trapezius engagement. Some patients may unknowingly lift their scapulae up and forward by engaging the levator scapulae muscle, with sequelar downward scapular rotation. The patient experienced almost immediate remission of her symptoms that were related to loading and articulation of the arms after learning to hold her shoulders up. Also note the trapezius hypertrophy, although the muscle is clearly not over-engaging in lifting the scapulae in the “before” image. This can be misleading, which is why scapular height must be measured rather than ‘eyeballed’.

Figure 2: TOS patient with severely depressed scapulae, before correction

Figure 3: TOS patient after correction
DISCUSSION
It has been suggested by several authours hthat the upper trapezius is overactive in patients with SIS and SD, based on EMG test results during glenohumeral articulation.17,44,47,129-131 Yet, despite this, a conspicuous pattern of scapular downward rotation, anterior tilting and protraction is demonstrated in the very same patients. Because the UT promotes upwards rotation and posterior tilting, as well as retraction,15,35,132 the notion that the UT is truly over-engaging in scapular movement does not seem likely. Contrary to this, the levator scapuli muscle will cause scapular elevation, protraction, downward rotation and anterior tilting,132-133 and is, therefore, a culprit more compatible with the evidence, than that of the UT. Moreover, regarding the authenticity of the documented excess UT EMG results, some studies show that hypertrophied muscles with high EMG output on the symptomatic side (in this case, the symptomatic sacroiliac side), was later proven to be significantly weak,134-136 and that the excessive EMG output signal normalized after increasing the respective muscle’s strength. This may suggest that it is not as black and white as the studies which demonstrate UT overactivity suggest; it may still be weak. A weak UT attempting to stabilize and move the scapulae properly, yet fails to do so, may explain why we see increased EMG signals in the UT yet movements which contradict its true involvement, i.e. movements of downward rotation, protraction, depression, which would not be reasonably present if there was legitimate over-engagement of the UT in scapular movement.
Other researchers suggest that in order to maintain proper scapular position during glenohumeral articulation, all of the stabilizers must engage, especially the UT, SA, middle trapezius and lower trapezius.11,60 It has also been stated that a common error is to over-engage the rhomboid by squeezing the shoulder blades together, as this will promote anterior scapular tilt with concomitant depression of the scapula by the latissimus dorsi muscle.11
In accordance with Watson and Mckinnon’s papers,11,60 I have experienced that by setting a patient into the norms that were provided by Sahrmann and others,6,10,11,14,16,34,44,46- one will quickly realize that most patients with neck and shoulder problems tend to have depressed scapulae, and that they need to engage their upper trapezius, not suppress it. A main muscle that retracts and upwardly rotates the scapula, is also the upper trapezius muscle. Most of the negative biomechanical associations (scapular downward rotation, anterior tilt, protraction, depression) with SD, SIS, and TOS, are functionally countered by the upper trapezius, which promote elevation, retraction, posterior tilting and upward rotation. Based on this, and the evidence considered, it would seem quite contraindicated to pull the scapula back and down. It has been demonstrated that scapular elevation has an immediate beneficial effect on cervical pain137 as well as range of motion.138 Further, it has been documented that subjects with lower scapular resting position have a tendency of higher pain thresholds in the upper trapezius.52–53 Whiplash associated disorders (WAD) patients have also been demonstrated to have low-riding clavicles.15,37 And, it has been demonstrated that patients with slouched scapulothoracic postures have decreased shoulder abduction ROM and posterior scapular tilting as well as decreased muscle force in glenohumeral abduction above 90˚.49 Finally, it has even been documented that patients with upper extremity deep vein thrombosis have a significantly narrower costoclavicular space in resting posture than that of controls.94,95 These would all make some solid points against pulling the clavicles back and down as postural means of therapeutic intervention.
Between January 1st 2017 and June 20th 2018, I evaluated 115 TOS patients for the co-presence of scapular depression, at my clinic in Oslo (Norway). They were diagnosed based on the criteria provided by Selmonosky’s diagnostic triad (DT) which involves supraclavicular tenderness (Morley’s sign) as well as relative weakness of the fifth finger, with or without a white hand sign.69,70,71,116 I classified scapular depression as having the superior scapular angle situated more than two finger widths below the T2 vertebra (approximately 2 cm). The survey revealed that 100% of the patients had scapular depression on the symptomatic side, cf. Sahrmann and colleagues’ norms. Most of these had been told to pull their scapulae back and down to correct their posture by their musculoskeletal therapist, and became considerably worse after following these cues, as a result. Five of these even had TOS surgery to decompress the CCS, but were still told to pull their shoulders back and down by their therapist, although TOS surgery clearly aims to increase the costoclavicular interval. The latter patients had severely depressed scapulae on the afflicted side, resulting in compression of brachial plexus between the clavicle and the 2nd rib. It is my impression, although clearly well-intended, that being cued to pull “back and down” obliviously and iatrogenically exacerbated the situation for these patients.
Because of the consensus that scapula has a tendency to protract, rotate forward (anterior tilt) and down (downward rotation) in patients with SD, SIS and neck pain, there may be some warrant in increasing scapular retraction alone. However, pulling back and down will cause the scapula to retract, depress and downwardly rotate, and is not compatible with any the criteria provided by the evidence, which states to increase retraction, upward rotation and posterior tilt. Increasing depression, downward rotation and anterior tilting may not only promote scapular dyskinesis and shoulder impingement syndrome, but also encroachment of the costoclavicular space and sequelar TOS.
The notion that proper scapular posture is obtained by pulling the shoulders back and down, is most likely based on only a few EMG studies, which show high upper trapezius output, as well as “pirate tales” from fitness and powerlifting communities. However, because patients with SIS and SD also demonstrate downward rotation, protraction, and depression, and, because the UT prevents these, it is unlikely to be truly over active nor over-engaged in moving the scapulae in a pathological manner. Retraction and depression of the scapulae may cause compression of the CCS as it mimics the Halstead’s CCS compression test. CCS compression implies osseous compression of the neurovascular bundle, which may lead to many diffuse and seemingly unrelated secondary problems, whose etiology may prove difficult to identify. Scapular depression has also been uniformly identified in TOS patients. There are also reports that scapular depression has been associated with increased myofascial pain in the cervical musculature, restricted range of motion, WAD, upper extremity DVT development, and more.
Therefore, often well-intended yet misunderstood cueing of pulling the shoulders “back and down”, may set the patient on a dark journey with many diffuse symptoms and few answers. Because unreliable diagnostic value of neurographic examinations, and because relatively few practitioners are versed in recognizing the signs of TOS, especially in its beginning-intermediate stages, there is likelihood that the patient will continue to pull their shoulders back and down and not suspect this as the etiology of their newfound problems. This can lead to longstanding problems for the patient and it may take a long time before his or her symptoms are finally identified as related to costoclavicular space compression.
LIMITATIONS
The survey part of this manuscript is based on patients who, on their own initiative have visited my unsubsidized private clinical practice. They may or may not fully represent the general patient population within the NHS.
CONCLUSION
In conclusion, it is of utmost importance to evaluate the patient’s scapular resting position based on the evidence, rather than generically cueing him or her to pull their scapulae back and down. If the patient presently has low-riding scapulae, and is cued further into depression, an iatrogenic sequela of maladies may develop as result. Pulling the shoulders “back and down” is a logical fallacy, which does not result in what it is thought to do, is not compatible with the evidence, the anatomy, biomechanics nor with common sense. Although the cue itself, and I reiterate, is clearly originating from well-meaning therapists, it is my impression that the SIS and SD studies have been gravely misinterpreted, and that the “back and down” cue should be abolished once and for all.
Conflict of interest
Nil
REFERENCES
- Osar, Evan. Forward shoulder posture and scapular retraction exercises. Accessed 2018 June 24. Available from https://www.otpbooks.com/evan-osar-forward-shoulder-posture/
- Scapular stabilisation exercises. Accessed 2018 June 24. Available from https://physioworks.com.au/treatments-1/scapular-stabilisation-exercises.
- Senger, Megan. Correct Cues for Scapular Motion. Accessed 2018 June 24. Available from https://www.acefitness.org/certifiednewsarticle/2384/correct-cues-for-scapular-motion/
- Bolton, Andy. How to break bench records. Accessed 2018 June 24. Available from https://www.t-nation.com/training/how-to-break-bench-records.
- Austin, Dan. Powerlifting. Human Kinetics Publishers; 2012.
- Osar, E. Corrective exercise solution to common hip and shoulder dysfunction. Lotus Publishers; 2012.
- Starkey C, Brown SD. Orthopedic & Athletic Injury Examination Handbook. 3rd edition. F.A. Davis Company; 2015.
- Magee DJ. Orthopedic physical assessment. 6th Elsevier; 2013.
- Mohindra M, Jain JK. Fundamentals of Orthopedics. 2nd edition. Jaypee Brothers Medical Publishers; 2017
- Hoppenfield S. Physical examination of the spine and extremities. 1st edition. Thomas H, Illustrator. Hutton R, Collaborator. Prentice Hall; 1976.
- Watson LA, Pizzari T, Balster S. Thoracic outlet syndrome Part 2: conservative management of thoracic outlet. Man Ther. 2010 Aug;15(4):305-14. [PubMed] doi: 10.1016/j.math.2010.03.002
- Kai Y, Oyama M, Kurose S, Inadome T, Oketani Y, Masuda Y. Neurogenic thoracic outlet syndrome in whiplash injury. J Spinal Disord. 2001 Dec;14(6):487-93. [PubMed]
- Skandalakis JE, Mirilas P. Benign anatomical mistakes: the thoracic outlet syndrome. Am Surg. 2001 Oct;67(10):1007-10. [PubMed]
- Telford ED, Mottershead S. Pressure at the cervico-brachial junction; an operative and anatomical study. J Bone Joint Surg Br. 1948 May;30B(2):249-65. [PubMed]
- Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996 Aug;24(2):57-65. [PubMed] [Free full text]
- McClure PW, Michener LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001 May-Jun;10(3):269-77. [PubMed]
- Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000 Mar;80(3):276-91. [PubMed]
- Endo K, Ikata T, Katoh S, Takeda Y. Radiographic assessment of scapular rotational tilt in chronic shoulder impingement syndrome. J Orthop Sci. 2001;6(1):3-10. [PubMed]
- Hébert LJ, Moffet H, McFadyen BJ, Dionne CE. Scapular behavior in shoulder impingement syndrome. Arch Phys Med Rehabil. 2002 Jan;83(1):60-9. [PubMed]
- Lin JJ, Lim HK, Yang JL. Effect of shoulder tightness on glenohumeral translation, scapular kinematics, and scapulohumeral rhythm in subjects with stiff shoulders. J Orthop Res. 2006 May;24(5):1044-51. [PubMed]
- Lawrence RL, Braman JP, Laprade RF, Ludewig PM. Comparison of 3-dimensional shoulder complex kinematics in individuals with and without shoulder pain, part 1: sternoclavicular, acromioclavicular, and scapulothoracic joints. J Orthop Sports Phys Ther. 2014 Sep;44(9):636-45, A1-8. doi: 10.2519/jospt.2014.5339. [PubMed] [Free full text]
- Warner JJ, Micheli LJ, Arslanian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moiré topographic analysis. Clin Orthop Relat Res. 1992 Dec;(285):191-9. [PubMed]
- Watson L, Balster SM, Finch C, Dalziel R. Measurement of scapula upward rotation: a reliable clinical procedure. Br J Sports Med. 2005 Sep;39(9):599-603. [PubMed] [Free full text]
- Struyf F, Nijs J, Baeyens JP, Mottram S, Meeusen R. Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand J Med Sci Sports. 2011 Jun;21(3):352-8. doi: 10.1111/j.1600-0838.2010.01274.x. [PubMed]
- Struyf F, Nijs J, De Graeve J, Mottram S, Meeusen R. Scapular positioning in overhead athletes with and without shoulder pain: a case-control study. Scand J Med Sci Sports. 2011 Dec;21(6):809-18. doi: 10.1111/j.1600-0838.2010.01115.x. [PubMed]
- Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38. [PubMed]
- Lukasiewicz AC, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999 Oct;29(10):574-83; discussion 584-6. [PubMed] [Free full text]
- Green RA, Taylor NF, Watson L, Ardern C. Altered scapula position in elite young cricketers with shoulder problems. J Sci Med Sport. 2013 Jan;16(1):22-7. doi: 10.1016/j.jsams.2012.05.017. [PubMed]
- Ludewig PM, Braman JP. Shoulder Impingement: biomechanical Considerations in Rehabilitation. Man Ther. 2011;16(1):33-39. doi:10.1016/j.math.2010.08.004. [PubMed] [Free full text]
- Greenfield B, Catlin PA, Coats PW, Green E, McDonald JJ, North C. Posture in patients with shoulder overuse injuries and healthy individuals. J Orthop Sports Phys Ther. 1995 May;21(5):287-95. [PubMed] [Free full text]
- Roche SJ, Funk L, Sciascia A, Kibler WB. Scapular dyskinesis: the surgeon’s perspective. Shoulder Elbow. 2015 Oct;7(4):289-97. doi: 10.1177/1758573215595949. [PubMed] [Free full text]
- Smith J, Dietrich CT, Kotajarvi BR, Kaufman KR. The effect of scapular protraction on isometric shoulder rotation strength in normal subjects. J Shoulder Elbow Surg. 2006 May-Jun;15(3):339-43. [PubMed]
- Borstad JD. Resting position variables at the shoulder: evidence to support a posture-impairment association. Phys Ther. 2006;86:549–57. [PubMed]
- Ludewig PM, Reynolds JF. The Association of Scapular Kinematics and Glenohumeral Joint Pathologies. J Orthop Sports Phys Ther. 2009 Feb; 39(2): 90–104. doi: 10.2519/jospt.2009.2808 [PubMed] [Free full text]
- Ludewig PM, Cook TM. The effect of head position on scapular orientation and muscle activity during shoulder elevation. J Occup Rehabil. 1996 Sep;6(3):147-58. doi: 10.1007/BF02110752. [PubMed]
- Helgadottir H, Kristjansson E, Mottram S, Karduna AR, Jonsson H Jr. Altered scapular orientation during arm elevation in patients with insidious onset neck pain and whiplash-associated disorder. J Orthop Sports Phys Ther. 2010;40:784–91. doi: 10.2519/jospt.2010.3405. [PubMed] [Free full text]
- Helgadottir H, Kristjansson E, Mottram S, Karduna A, Jonsson H Jr. Altered alignment of the shoulder girdle and cervical spine in patients with insidious onset neck pain and whiplash-associated disorder. J Appl Biomech. 2011;27:181–91. [PubMed]
- Martínez-Merinero P, Lluch E, Gallezo-Izquierdo T, Pecos-Martín D, Plaza-Manzano G, Nuñez-Nagy S, et al. The influence of a depressed scapular alignment on upper limb neural tissue mechanosensitivity and local pressure pain sensitivity. Musculoskelet Sci Pract. 2017 Jun;29:60-65. doi: 10.1016/j.msksp.2017.03.001. [PubMed]
- Azevedo DC, de Lima Pires T, de Souza Andrade F, McDonnell MK. Influence of scapular position on the pressure pain threshold of the upper trapezius muscle region. Eur J Pain. 2008 Feb;12(2):226-32. [PubMed]
- Kibler WB. Scapular involvement in impingement: signs and symptoms. Instr Course Lect. 2006;55:35-43 [PubMed]
- Struyf F1, Nijs J, Mottram S, Roussel NA, Cools AM, Meeusen R. Clinical assessment of the scapula: a review of the literature. Br J Sports Med.2014 Jun;48(11):883-90. [PubMed] doi:10.1136/bjsports-2012-091059
- Kaur K, Das PG, Lenka PK, Anwer S. Immediate effect of posture correction of trapezius activity in computer users having neck pain – an electromyographic analysis. The Internet Journal of Allied Health Sciences and Practice. 2013 Oct 01;11(4), Article 10 [Free full text]
- Tate A, McClure P, Kareha S, Irwin D. Effect of the scapula reposition test on shoulder impingement symptoms and elevation strength in overhead athletes. J Orthop Sports Phys Ther. 2008;38:4–11. [PubMed] [Free full text]
- Kendall FP, McCreary EK, Provance PG. Muscles: Testing and Function with Posture and Pain. Williams and Wilkins. 4thBaltimore.1993;pp 286–293
- Swift TR, Nichols FT. The droopy shoulder syndrome. Neurology. 1984 Feb;34(2):212-5 [PubMed]
- Todd TW. The Descent of the Shoulder after Birth. Anat. Anz. Bd. Aufsatze. 1912:41(14):385-97
- Sahrmann, S.A. Diagnosis and Treatment of Movement Impairment Syndrome. St. Louis:Mosby;2002. 30-31p.
- Sahrmann S. Movement System Impairment Syndromes of the Extremities, Cervical and Thoracic Spines. Elsevier Health Sciences; 2010.
- Kebaetse M, McClure P, Pratt NA. Thoracic position effect on shoulder range of motion, strength, and three-dimensional scapular kinematics. Arch Phys Med Rehabil. 1999 Aug;80(8):945-50. [PubMed] [Free full text]
- Wijeratna MD, Troupis JM, Bell SN. The use of four-dimensional computed tomography to diagnose costoclavicular impingement causing thoracic outlet syndrome. Shoulder Elbow. 2014;6(4):273–75 [PubMed] [Free full text] DOI: 10.1177/1758573214533781
- Walsh MT. Therapist management of thoracic outlet syndrome. J Hand Ther. 1994 Apr-Jun;7(2):131-44. [PubMed]
- Kenny RA, Traynor GB, Withington D, Keegan DJ. Thoracic outlet syndrome: a useful exercise treatment option. Am J of Surgery.1993;165(2):282-84. [Link]
- Press JM, Young JL. Vague upper-extremity symptoms? Phys Sportsmed. 1994 Jul;22(7):57-64 [PubMed] doi: 10.1080/00913847.1994.11947668.
- Pascarelli EF, Hsu YP. Understanding work-related upper extremity disorders: clinical findings in 485 computer users, musicians, and others. J Occup Rehabil. 2001;11(1):1e21. [PubMed]
- Ranney D. Thoracic outlet: an anatomical redefinition that makes clinical sense. Clin Anat. 1996;9(1):50-2. [PubMed]
- Sucher BM. Thoracic outlet syndromeea myofascial variant: part 2. Treatment. J Am Osteopath Associ.1990;90(9):810-2, 817-823. [PubMed] [Free full text]
- Aligne C, Barral X. Rehabilitation of patients with thoracic outlet syndrome. Ann Vasc Surg. 1992;6(4):381e9. [PubMed]
- Kitamura T, Takagi K, Yamaga M, Morisawa K. Brachial plexus stretching injuries: microcirculation of the brachial plexus. J Shoulder Elbow Surg. 1995;4(2):118-23. [PubMed]
- Thompson, R.W. Neurogenic TOS. Accessed 2016 March 15. Available at http://tos.wustl.edu/What-is-TOS/Types-of-TOS/Neurogenic-TOS.
- Mackinnon SE, Novak CB. Thoracic outlet syndrome. Curr Probl Surg. 2002;39(11):1070-145. [PubMed]
- Kieffer E. Actualités de chirurgie vasculaire. Les syndromes de la traversée thoraco-brachiale. Paris: A.E.R.C.V. éditions; 1989. [Free full text]
- Merle M. Les syndromes de la traversée cervico-thoraco-brachiale. Monographie des Annales de Chirurgie de la Main. 1995;7:29–47. [Free full text]
- Alexandre J, Le Dû C, Corcia P, Laulan J. Formes déficitaires du syndrome de la traversée thoraco-brachiale. A propos de 16 cas. 41e congrès du GEM; Paris, décembre. 2005.
- Allieu Y, Benichou M, Touchais S, Desbonnet P, Lussiez B. Les formes neurologiques du syndrome du hile du membre supérieur: le rôle du scalène moyen. Ann Chir Main. 1991;10:308–312
- Laulan J, Fouquet B, Rodaix C, Jauffret P, Roquelaure Y, Descatha A. Thoracic outlet syndrome: definition, aetiological factors, diagnosis, management and occupational impact. J Occup Rehabi. 2011;21(3):366-73. doi:10.1007/s10926-010-9278-9. [PubMed] [Free full text]
- Dahlin LB, Lundborg G. The neurone and its response to peripheral nerve compression. J Hand Surg. 1990;15(1):5–10. [PubMed]
- Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet. 1973;2:359–62. [PubMed]
- Narakas AO. The role of thoracic outlet syndrome in the double crush syndrome. Ann Chir Main Memb Super. 1990;9:331–40. [PubMed]
- Selmonosky CA, Byrd R, Blood C, Blanc JS. Useful triad for diagnosing the cause of chest pain. South Med J. 1981; 74:947-49. [PubMed]
- Selmonosky CA. The white hand sign. A new single maneuver useful in the diagnosis of thoracic outlet syndrome. Southern Med Journal. 2002; 85:557. [Abstract]
- Selmonosky CA, Poblete Silva R. The diagnosis of thoracic outlet syndrome. Myths and Facts. Chilean J of Surg. 2008 June; 60(3):255-261.
- Sanders RJ, Hammond SL, Rao NM. Thoracic outlet syndrome: a review. Neurologist. 2008 Nov;14(6):365-73. [PubMed] doi: 10.1097/NRL.0b013e318176b98d.
- Durham JR, Yao JS, Pearce WH, Nuber GM, McCarthy WJ 3rd. Arterial injuries in the thoracic outlet syndrome. J Vasc Surg. 1995 Jan;21(1):57-69; discussion 70. [PubMed]
- Chen D, Gu Y, Lao J, Chen L. Dorsal scapular nerve compression. Atypical thoracic outlet syndrome. Chin Med J. 1995;108:582-5 [PubMed]
- Akgun K, Aktas I, Terzi Y. Winged scapula caused by a dorsal scapular nerve lesion: a case report. Arch Phys Med Rehabil. 2008;89:2017-20. [PubMed] doi: 10.1016/j.apmr.2008.03.015.
- Aralasmak A, Karaali K, Cevikol C, Uysal H, Senol U. MR Imaging Findings in Brachial Plexopathy with Thoracic Outlet Syndrome. American Journal of Neuroradiology. 2010 March;31(3):410-417. [Free full text]
- Riddell DH, Smith BM. Thoracic and vascular aspects of thoracic outlet syndrome. Clin Orthop. 1986;207:31–6. [Abstract]
- Foley JM, Finlayson H, Travlos A. A Review of thoracic outlet syndrome and the possible role of botulinum toxin in the treatment of this syndrome. Toxins. 2012;4(11):1223-35. [PubMed] [Free full text] doi:10.3390/toxins4111223
- Hooper TL, Denton J, McGalliard MK, Brismée JM, Sizer PS Jr. Thoracic outlet syndrome: a controversial clinical condition. Part 1: anatomy, and clinical examination/diagnosis. J Man Manip Ther. 2010 Jun;18(2):74-83. [PubMed] [Free full text] doi: 10.1179/106698110X12640740712734
- Sanders RJ, Hammond SL, Rao NM. Diagnosis of thoracic outlet syndrome. J Vasc Surg. 2007 Sep;46(3):601-4. [PubMed]
- Archie M, Rigberg D. Vascular TOS—Creating a Protocol and Sticking to It. Diagnostics. 2017;7(2):34. [PubMed] doi:10.3390/diagnostics7020034.
- Pemberton, HS. Sign of submerged goitre. Lancet. 1948;248:509. doi:10.1016/s0140-6736(46)91790-4
- Sina F, Razmeh S, Habibzadeh N, Zavari A, Nabovvati M. Migraine headache in patients with idiopathic intracranial hypertension. Neurol Int. 2017;9(3):7280. doi:10.4081/or.2017.7280. [PubMed] [Free full text]
- De Simone R, Ranieri A, Montella S, et al. Intracranial pressure in unresponsive chronic migraine. J Neurol. 2014;261: 1365-73. [PubMed] [Free full text]
- Ninan T. Mathew, K. Ravishankar, Luis C. Sanin. Coexistence of migraine and idiopathic intracranial hypertension without papilledema. Neurology. 1996;46(5):1226-30. [PubMed]
- Yri HM, Rönnbäck C, Wegener M, Hamann S, Jensen RH. The course of headache in idiopathic intracranial hypertension: a 12-month prospective follow-up study. Eur J Neurol. 2014;21:1458–64. doi:10.1111/ene.12512 [PubMed]
- Ozdemir O, Ozcakar L. Thoracic outlet syndrome: Another cause for unilateral palmar hyperhidrosis. Clin Rheumatol. 2007;26(8):1375-76. [PubMed]
- Suderland S, ed. Nerve Injury. 2nd ed. NY:Edinburg NY Churchill Livingston; 1970 [1981 Printing].
- Urschel Jr HC, Razzuk MA. Upper plexus thoracic outlet syndrome: optimal therapy. Ann Thorac Surg. 1997;63(4):935-39. [Free full text]
- Urschel HC Jr, Kourtis H, Jr. Thoracic outlet syndrome: a 50 year experience at Baylor University. Proc (Bayl Union Med Cent).2007;20(2):125-35. [PubMed] [Free full text]
- Urschel HC, Razzuk MA, Hyland JW, Matson JL, Solis RA, Wood RE, et al. Thoracic outlet syndrome masquerading as coronary artery disease (pseudoangina). Ann Thorac Surg.1973;16(3):239-48 [Abstract]
- Vemuri C, McLaughlin LN, Abuirqeba AA, Thompson RW. Clinical presentation and management of arterial thoracic outlet syndrome. J Vasc Surg. 2017;65(5):1429-39 [Free full text]
- Shreeve MW, La Rose JR. Chiropractic care of a patient with thoracic outlet syndrome and arrhythmia. J Chiropr Med.2011;10(2):130-34 [PubMed] [Free full text] doi: 1016/j.jcm.2010.09.002
- Yamagami T, Handa H, Higashi K, Kaji R. Brachial plexus injury with cough attack: case report. Neurosurgery. 1994;34(6):1084-6; discussion 1086. [PubMed]
- Arnhjort T, Nordberg J, Delle M, Borgis CJ, Rosfors S, Larfars G. The importance of the costoclavicular space in upper limb primary deep vein thrombosis, a study with magnetic resonance imaging (MRI) technique enhanced by a blood pool agent. Eur J Intern Med. 2014;25(6):545-49. [PubMed] [Free full text]
- Fiorentini C, Mattioli S, Graziosi F, Bonfiglioli R, Armstrong TJ, Violante FS. Occupational relevance of subclavian vein thrombosis in association with thoracic outlet syndrome. Scand J Work Environ Health. 2005;31:160–163. [PubMed]
- Olin T.(1961) Arterial Complications in Thoracic Outlet Compression Syndrome, Acta Radiologica. 1961;56:97-112 [Free full text] , DOI: 10.3109/00016926109176643
- Lee TS, Hines GL. Cerebral embolic stroke and arm ischemia in a teenager with arterial thoracic outlet syndrome: a case report. Vasc Endovascular Surg. 2007;41(3):254-57 [PubMed]
- Palmer OP, Weaver FA. Bilateral cervical ribs causing cerebellar stroke and arterial thoracic outlet syndrome: a case report and review of the literature. Ann Vasc Surg.2015;29(4)840.e1-4 [PubMed] doi: 10.1016/j.avsg.2014.12.008.
- Boezaart AP, Haller A, Laduzenski S, Koyyalamudi VB, Ihnatsenka B, Wright T. Neurogenic thoracic outlet syndrome: A case report and review of the literature. Int J Shoulder Surg. 2010;4(2):27-35. doi:10.4103/0973-6042.70817. [PubMed] [Free full text]
- Atasoy E. Thoracic outlet compression sydnrome. Orthop Clin North Am. 1996;27(2):265-303. [PubMed]
- Povlsen B, Hansson T, Povlsen SD. Treatment for thoracic outlet syndrome. Cochrane Database Syst Rev. 2014 Nov 26;(11):CD007218. doi: 10.1002/14651858.CD007218.pub3. [PubMed]
- Redman L, Robbs J. Neurogenic thoracic outlet syndrome: Are anatomical anomalies significant? S Afr J Surg. 2015 Oct 8;53(1):22-5. [PubMed] [Free full text]
- Köknel TG. Thoracic outlet syndrome. Agri. 2005 Apr;17(2):5-9. [PubMed] [Free full text]
- Robey JH, Boyle KL. Bilateral Functional Thoracic Outlet Syndrome in a Collegiate Football Player. N Am J Sports Phys Ther. 2009 Nov; 4(4): 170–81. [PubMed] [Free full text]
- Tolson TD. “EMG” for thoracic outlet syndrome. Hand Clin. 2004;20: 37– 42. [PubMed]
- Passero S, Paradiso C, Giannini F, Cioni R, Burgalassi L, Battistini. Diagnosis of thoracic outlet syndrome. Relative value of electrophysiological studies. Acta Neurol Scand. 1994;90:179–85. [PubMed]
- Tsao BE, Ferrante MA, Wilbourn AJ, Shields RW. Electrodiagnostic features of true neurogenic thoracic outlet syndrome. Muscle Nerve. 2014;49(5):724-27 [PubMed] doi: 10.1002/mus.24066.
- Veilleux M, Stevens JC, Campbell JK. Somatosensory evoked poten- tials: lack of value for diagnosis of thoracic outlet syndrome. Muscle Nerve. 1988;11:571–75. [PubMed]
- Aminoff MJ, Olney RK, Parry GJ, Raskin NH. Relative utility of different electrophysiologic techniques in the evaluation of brachial plexopathies. Neurology. 1988;38:546–50. [PubMed]
- Komanetsky RM, Novak CB, Mackinnon SE, Russo MH, Padberg AM, Louis S. Somatosensory evoked potentials fail to diagnose thoracic outlet syndrome. J Hand Surg Am. 1996 Jul;21(4):662-6. [PubMed]
- Rousseff R, Tzvetanov P, Valkov I. Utility (or futility?) of electrodiagnosis in thoracic outlet syndrome. Electromyogr Clin Neurophysiol. 2005 Apr-May;45(3):131-33. [PubMed]
- Kwee RM, Chhabra A, Wang KC, Marker DR, Carrino JA. Accuracy of MRI in diagnosing peripheral nerve disease: a systematic review of the literature. Am J Roentgenol.2014;203:1303-09 [PubMed] [Free full text]
- Sanders RJ, Annest SJ. Pectoralis Minor Syndrome: Subclavicular Brachial Plexus Compression. Diagnostics. 2017;7(3):46. [PubMed] [Free full text] doi:10.3390/diagnostics7030046
- Brantigan CO, Roos DB. Diagnosing thoracic outlet syndrome. Hand Clin. 2004;20:27–36. [PubMed] [Free full text]
- Liu JE, Tahmoush AJ, Roos DB, Schwartzman RJ. Shoulder-arm pain from cervical bands and scalene muscle anomalies. J Neurol Sci. 1995;128:175–80 [PubMed]
- Selmonosky, C.A. Diagnosis of Thoracic Outlet Syndrome. Accessed on 2015 May 15. Available at http://www.tos-syndrome.com.
- Fried, SM. Nazarian LN. Dynamic neuromusculoskeletal ultrasound documentation of brachial plexus/thoracic outlet compression during elevated arm stress testing. Hand (NY) 2013;8:358-365, [PubMed] [Free full text] doi: 10.1007/s11552-013-9523-8
- Braun RM. Rechnic M. Shah KN. Pulse oximetry measurements in the evaluation of patients with possible thoracic outlet syndrome. J Hand Surg Am. 2012;37:2564-69. [PubMed] doi: 10.1016/j.jhsa.2012.09.020
- Thompson RW. Bryan’s Story. Accessed on 2016 March 3. Available at http://tos.wustl.edu/Patient-Features/Bryans-Story.
- Illig KA, Doyle AJ. A comprehensive review of Paget-Schroetter syndrome. J Vasc Surg. 2010;51:1538-47
[PubMed] [Free full text] Doi:10.1016/j.jvs.2009.12.022
- Guzzo JL, Chang K, Demos J, Black JH, Freischlag JA. Preoperative thrombolysis and venoplasty affords no benefit in patency following first rib resection and scalenectomy for subacute and chronic subclavian vein thrombosis. J Vasc Surg. 2010;52(3):658-62 [PubMed] doi: 10.1016/j.jvs.2010.04.050
- Laudner KG, Stanek JM, Meister K. Differences in scapular upward rotation between baseball pitchers and position players. Am J Sports Med. 2007 Dec;35(12):2091-5 [PubMed] doi: org/10.1177/0363546507305098
- Johnson MP, McClure PW, Karduna AR. New method to assess scapular upward rotation in subjects with shoulder pathology. J Orthop Sports Phys Ther. 2001 Feb;31(2):81-9. [PubMed] [Free full text]
- Borsa PA, Timmons MK, Sauers EL. Scapular-positioning patterns during humeral elevation in unimpaired shoulders. J Athl Train. 2003;38(1):12-17. [Free full text]
- Su KP, Johnson MP, Gracely EJ, Karduna AR. Scapular rotation in swimmers with and without impingement syndrome: practice effects. Med Sci Sports Exerc. 2004 Jul;36(7):1117-23. [PubMed]
- Scibek JS, Carcia CR. Validation of a new method for assessing scapular anterior‐posterior tilt. Int J Sports Phys Ther. 2014 Oct;9(5):644–56. [PubMed] [Free full text]
- Shobush DC, Simoneau GG, Dietz KE, Levene JA, Grossman RE, Smith WB . The Lennie test for measuring scapular position in healthy young adult females: a reliability and validity study. J Orthop Sports Phys Ther. 1996;23(1):39-50. [PubMed] [Free full text]
- O’Shea A, Kelly R, Williams S, McKenna L. Reliability and Validity of the Measurement of Scapular Position Using the Protractor Method. Phys ther. 2016;96(4):502 [PubMed] doi: 10.2522/ptj.20150144.
- Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003 May;33(5):247-58. [PubMed] [Free full text]
- Cools AM, Witvrouw EE, Declercq GA, Vanderstraeten GG, Cambier DC. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction–retraction movement in overhead athletes with impingement symptoms Br J Sports Med. 2004;38:64-68 [Free full text]
- Cools AM, Declercq GA, Cambier DC, Mahieu NM, Witvrouw EE. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scand J Med Sci Sports. 2007 Feb;17(1):25-33 [PubMed]
- Paine R, Voight ML. The role of the scapula. Int J Sports Phys Ther. 2013;8(5):617–29. [PubMed] [Free full text]
- Reinold MM, Escamilla R, Wilk KE. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009;39:105–117 [PubMed] [Free full text] doi: 10.2519/jospt.2009.2835.
- Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat. 2012;221(6):537-67. [PubMed] [Free full text] doi:10.1111/j.1469-7580.2012.01564.x.
- Mooney V, Pozos R, Vleeming A, Gulick J, Swenski D. Exercise treatment for sacroiliac pain. Orthopedics. 2001 Jan;24(1):29-32. [PubMed]
- Massoud Arab A, Reza Nourbakhsh M, Mohammadifar A. The relationship between hamstring length and gluteal muscle strength in individuals with sacroiliac joint dysfunction. J Man Manip Ther. 2011 Feb;19(1):5-10 [PubMed] [Free full text]doi:10.1179/106698110X12804993426848.
- Van Dillen LR, McDonnell MK, Susco TM, Sahrmann SA. The immediate effect of passive scapular elevation on symptoms with active neck rotation in patients with neck pain. Clin J Pain. 2007 Oct;23(8):641-7. [PubMed]
- Andrade GT, Azevedo DC, De Assis Lorentz I, Galo Neto RS, Sadala Do Pinho V, Ferraz Goncalves RT, et al. Influence of scapular position on cervical rotation range of motion. J Orthop Sports Phys Ther. 2008 Nov;38(11):668-73. [PubMed] [Free full text]
![21-OA-Fig1]()