↧
Obituary
↧
A comparative study of intraperitoneal ropivacaine and bupivacaine for postoperative analgesia in laparoscopic cholecystectomy: a randomized controlled trial
Rajesh Kumar Meena1*, Kavita Meena2, Sandeep Loha1, Shashi Prakash3
1Assistant professor; 2Senior resident; 3Associate professor
Department of Anaesthesiology, Institute of Medical Sciences, Banaras Hindu University (BHU), Varanasi, Uttar Pradesh 221005, (India)
Correspondence: Dr Rajesh Kumar Meena, Department of Anaesthesiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh 221005, (India): E-mail: drrajaiims86@gmail.com: Phone: 0 9455231072
ABSTRACT
Introduction: Laparoscopic cholecystectomy is now the gold standard for treatment of symptomatic gallstones. After this surgery patients suffer visceral and shoulder pain secondary to peritoneal insufflation. Use of intraperitoneal and port site instillation of local anesthetics has been used to reduce postoperative pain and decreases the need for intravenous opioids. Studies regarding comparison of intraperitoneal use of ropivacaine and bupivacaine to reduce postoperative pain are few. This study compared the efficacy of ropivacaine and bupivacaine in reducing postoperative pain after laparoscopic cholecystectomy.
Methodology: After ethical committee’s clearance and informed consent 100 patients with symptomatic cholelithiasis, aged 20-70 years, of either gender, ASA status I to III and within ± 20% of ideal body weight, scheduled for laparoscopic cholecystectomy were included. . Patients were randomized into two groups with 50 patients in each group.
Group-B: Patients received 0.5% bupivacaine in a dose of 2 mg/kg diluted in normal saline to make a solution of 50 ml.
Group-R: Patients received 0.75% ropivacaine in a dose of 2 mg/kg diluted in normal saline to make a solution of 50 ml.
Drug was instilled intra-peritoneal through in situ placed infra-umbilical trocar before extubation. NIBP, HR, SpO2, VAS, verbal rating scale (VRS) and rescue analgesia were recorded immediately postoperatively and then regularly every hour for the next 12 hours.
Results: HR, SBP and DBP were comparatively lower in Group-R than in Group-B. The VAS score was significantly lower in Group-R from postoperative 5th hr to 12th hr. Rescue analgesia was given when VAS was > 40. VRS score was significantly lower in Group-R from postoperative 7th hr, showing longer duration of analgesia in this group. The rescue analgesia requirement was also less in Group-R.
Conclusion: We conclude that the instillation of bupivacaine and ropivacaine intraperitonelly is an effective method of postoperative pain relief in laparoscopic cholecystectomy. It provides good analgesia in immediate postoperative period with ropivacaine providing longer duration of analgesia.
Key words: Laparoscopic cholecystectomy; Intraperitoneal; Ropivacaine; Bupivacaine
Citation: Meena RK, Meena K, Loha S, Prakash S. A comparative study of intraperitoneal ropivacaine and bupivacaine for postoperative analgesia in laparoscopic cholecystectomy: a randomized controlled trial. Anaesth Pain & Intensive Care 2016;20(3):295-30
Received: 10 April 2016; Reviewed: 6 May 2016; Corrected: 23 My 2016; Accepted: 16 June 2016
INTRODUCTION
Laparoscopic cholecystectomy (LC) is now the gold standard treatment for symptomatic gallstones and is the commonest operation performed laparoscopically world-wide. The indications for its use in the treatment of gallstone are the same as open operation although the cholecystectomy rate has increased, since the introduction of laparoscopic technique.1
Although pain following LC is less intense than open surgery it can occur due to stretching of parietal peritoneum from insufflations of gas intraperitoneally, release of inflammatory mediators and irritation produced by blood. This can delay the patient’s autonomy; lengthen the hospital stay, and increase morbidity and costs. Multi modal analgesic techniques are therefore necessary to provide effective postoperative analgesia.2
Administration of intraperitoneal local anesthetic (LA), either during or after surgery, is used by many surgeons as a method of reducing postoperative pain. This technique was first evaluated in patients undergoing gynecological laparoscopic surgery by Narchi et al.3 Its application in LC was initially examined in a randomized trial in 1993 by Chundrigar et al.4 Since then, several trials evaluating the efficacy of intraperitoneal LA in LC have been published worldwide.5
The LA has been administered in different doses and at different sites with varying success.6 intraperitoneal administration of local anesthetic has not only proven to be effective in the relief of postoperative pain, but also reduces nausea and vomiting .7
Intraperitoneal use of LA decreases incidence of postoperative pain and the need for intravenous opioids. There have been encouraging results in recent studies using bupivacaine with NSAIDS and opioids.8
The objective of our study was to compare the efficacy of intraperitoneal bupivacaine and ropivacaine for postoperative pain relief and to observe for side effects.
METHODOLOGY
This randomized, blinded study included 100 patients with uncomplicated, symptomatic cholelithiasis admitted to general surgery department of IMS, BHU. Informed consent was obtained. All the investigated patients were managed by experienced surgeons. The study was approved by the institutional ethics committee of the institute. Patients were randomly divided into two groups. Inclusion criteria were age between 20-70 years, either gender, ASA physical status I to III, scheduled for LC. Patients with following underlying co-morbidities were excluded; coagulopathy, infection at local site, congestive heart failure, uncontrolled diabetes mellitus, respiratory distress, systemic infection, allergy to drugs used, emergency operation, history of malignancy, regular use of NSAIDS or any other analgesic, history of alcohol or drug abuse, confirmed local anesthetic toxicity, chronic pain syndrome, neurological disease and treatment with steroids prior to surgery.
At the time of pre-anesthetic check-up patient’s age, gender, height, weight, and relevant history were recorded. Patients were examined for airway assessment, blood pressure (systolic, diastolic and mean), heart rate, and other relevant systems. Patients were also instructed on the use of VSA.
Investigations included hemoglobin, urea, creatinine, total leucocytes count, fasting blood sugar, ECG, and chest x-ray. In the operating room, baseline heart rate, non-invasive arterial blood pressure, pulse oximetry and respiratory rate were recorded. 18G peripheral venous cannula was inserted on the dorsal side of the patient’s left hand, and 5 ml/kg Ringer’s lactate was preloaded. Patients were randomized into one of the two groups using a computer generated table of random numbers. Drug solution was prepared by a doctor who was not directly participating in the study. Drug was filled in pre-coded 50 ml syringe. Blinded solution was prepared in perioperative period procedure. Blinding was continued in postoperative period. Dose was chosen on bases of previous studies.
Group-B: Patients received 0.5% bupivacaine in a dose of 2 mg/kg diluted in normal saline to make a solution of 50 ml.
Group-R: Patients received 0.75% ropivacaine in a dose of 2 mg/kg diluted in normal saline to make a solution of 50 ml.13
All patients received ondansetron (0.1 mg/kg) intravenously half an hour prior to induction of anesthesia and fentanyl (2 µg/kg) intravenously just before induction. Surgery was carried out under general anesthesia with propofol (1-2.5 mg/kg) and vecuronium (0.12 mg/kg) to facilitate tracheal intubation. Anesthesia was maintained on 60% N2O in oxygen with 0.5 to 1% isoflurane. Adequate muscle relaxation was achieved with intermittent doses of vecuronium bromide (0.01 mg/kg). Ventilation (tidal volume 6-8 ml/kg) was adjusted to maintain end tidal carbon dioxide between 35 and 40 mmHg. Patients were placed in 15-20° reverse Trendelenburg position during surgery. During laparoscopy, intra-abdominal pressure was maintained at 12 mmHg. All surgeries were performed by the same experienced surgeon. The CO2 was carefully evacuated at the end of surgery by manual compression of the abdomen with open trocars. The drug was instilled intra-peritoneally through the infra-umbilical incision before removal of trocar at end of the surgery, by an experienced surgeon. Trendelenburg position was used to facilitate dispersion of drug solution in sub hepatic region. Patients were shifted to recovery room only after complete recovery from anesthesia. All patients were monitored for next 12 hours in post anesthesia care unit.
Non-invasive blood pressure, heart rate and peripheral oxygen saturation were recorded immediate postoperatively and then regularly every hour till next 12 hours. The following verbal rating pain scale was used
Verbal Rating Pain Scale (VRS)
Score 0: no pain and patient sedated
Score 1: patient awake and no pain on coughing
Score 2: pain on coughing but not on deep breathing
Score 3: pain on deep breathing but not at rest
Score 4: slight pain at rest
Score 5: severe pain at rest.
The degree of postoperative pain was assessed using both visual analogue scale (VAS) and VRS on arrival in the recovery room, immediately after surgery and thereafter one hourly till 12 hours postoperatively. Patients having VAS > 40 mm after surgery were administered a bolus of diclofenac aqueous (75 mg) IV as rescue analgesia. Ondansetron (0.1 mg/kg IV) was administered on complaint of nausea. Time to first analgesic requirement, total analgesic consumption in the first 12 hours postoperatively and occurrence of adverse events were also recorded. Patients were regularly asked about pruritus and shoulder pain, and blood pressure was monitored for episodes of hypotension (MAP < 60 mmHg), heart rate (HR) was monitored for episodes of bradycardia (HR < 60). Total duration of surgery was recorded in all the cases. All perioperative complications like biliary spillage, hemorrhage, intra-operative bradycardia, hypotension and hypertension were recorded.
Statistical analysis was done using SPSS for Windows version 16.0 software. For non-continuous data Chi-square test was used. The mean and standard deviation of the parameters studied during observation period were calculated for two treatment groups and compared using Student’s t-test. The critical value of ‘p’ indicating the probability of significant difference was taken as < 0.05.
RESULTS
Table 1 shows that mean age, height, weight and duration of surgery in the two groups which was comparable
Table 1: Demographic distribution
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
p-value |
| Age( yr) | 41.58 ± 14.574 | 43.64 ± 13.815 | 0.470 |
| Height( cm) | 162.76 ± 9.428 | 164.36 ± 8.647 | 0.379 |
| Weight( kg) | 65.24 ± 11.698 | 67.28 ± 10.581 | 0.363 |
| Duration of surgery( min) | 33.74 ± 10.766 | 30.30 ± 6.011 | 0.051 |
| Sex (M/F) | 16/34 | 21/39 | 0.300 |
Table 2 shows the comparison of mean heart rate in two groups at different intervals which showed that they were statistically significant (p < 0.05) from post-operative 1st hr to 9th hr. Afterwards, they were comparable and statistically non-significant. Heart rate was comparatively lower in Group-R than in Group-B in postoperative period.
Table 2: Comparison of heart rate in two groups (per min)
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| HR-baseline | 81.58 ± 7.659 | 83.64 ± 9.501 | -1.194 | 0.236 |
| HR-Immediate postop period | 85.92 ± 7.174 | 81.64 ± 14.470 | 1.874 | 0.064 |
| HR-1 | 80.94 ± 7.797 | 73.76 ± 13.602 | 3.238 | 0.002 |
| HR-2 | 84 ± 9.640 | 76.30 ± 14.305 | 3.189 | 0.002 |
| HR-3 | 88.34 ± 12.047 | 75.04 ± 15.712 | 4.750 | <0.001 |
| HR-4 | 79.02 ± 6.906 | 72.74 ± 13.585 | 2.914 | 0.004 |
| HR-5 | 79.36 ± 6.404 | 74.50 ± 12.500 | 2.447 | 0.016 |
| HR-6 | 79.70 ± 7.560 | 73.00 ± 11.350 | 3.474 | 0.001 |
| HR-7 | 81.06 ± 7.327 | 74.32 ± 11.133 | 3.576 | 0.001 |
| HR-8 | 81.14 ± 7.467 | 75.32 ± 9.584 | 3.387 | 0.001 |
| HR-9 | 81.20 ± 8.010 | 77.02 ± 11.188 | 2.148 | 0.034 |
| HR-10 | 79.30 ± 5.219 | 76.38 ± 10.721 | 1.732 | 0.086 |
| HR-11 | 79.88 ± 5.731 | 77.26 ± 10.762 | 1.519 | 0.132 |
| HR-12 | 79.80 ± 6.752 | 78.82 ± 8.324 | 0.647 | 0.519 |
Table 3 shows the comparison of mean systolic blood pressure in two groups at different intervals which showed that they were comparable and statistically non-significant (p < 0.05) except in the immediate post-operative period. Systolic blood pressure was comparatively lower in Group-R than in Group-B in postoperative period.
Table 3: Systolic blood pressure distribution (mmHg)
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| SBP-baseline | 123.00 ± 8.778 | 120.64 ± 14.787 | 0.970 | 0.334 |
| SBP-Immediate postoperative period | 132.00 ± 8.330 | 125.08 ± 12.873 | 3.191 | 0.002 |
| SBP-1 | 126.10 ± 9.679 | 124.28 ± 12.749 | 0.804 | 0.423 |
| SBP-2 | 121.36 ± 8.223 | 120.36 ± 12.753 | 466 | 0.642 |
| SBP-3 | 121.80 ± 9.100 | 118.46 ± 10.979 | 1.656 | 0.101 |
| SBP-4 | 120.24 ± 9.011 | 117.78 ± 0.332 | 1.269 | 0.208 |
| SBP-5 | 120.32 ± 8.163 | 117.54 ± 11.022 | 1.433 | 0.155 |
| SBP-6 | 119.74 ± 6.223 | 118.18 ± 9.983 | 0.938 | 0.351 |
| SBP-7 | 120.34 ± 7.345 | 119.54 ± 7.702 | 0.532 | 0.596 |
| SBP-8 | 120.06 ± 7.924 | 118.50 ± 9.511 | 0.891 | 0.375 |
| SBP-9 | 121.50 ± 11.603 | 119.20 ± 9.315 | 1.093 | 0.277 |
| SBP-10 | 117.88 ± 11.349 | 119.64 ± 10.129 | -.818 | 0.415 |
| SBP-11 | 119.82 ± 9.220 | 118.58 ± 9.498 | 0.662 | 0.509 |
| SBP-12 | 117.88 ± 9.410 | 121.00 ± 10.844 | -1.537 | 0.128 |
Table 4 shows the comparison of mean diastolic blood pressure in two groups at different intervals which showed that they were comparable and statistically non-significant (p < 0.05). Diastolic blood pressure was comparatively lower in Group-R than in Group-B in postoperative period
Table 4: Diastolic blood pressure (mmHg) distribution
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| DBP-baseline | 79.62 ± 5.739 | 78.84 ± 5.508 | 0.693 | 0.490 |
| DBP-Immediate postoperative period | 85.42 ± 5.507 | 83.76 ± 7.397 | 1.273 | 0.206 |
| DBP-1 | 80.04 ± 5.653 | 78.66 ± 10.481 | 0.819 | 0.415 |
| DBP-2 | 81.28 ± 7.778 | 79.96 ± 10.292 | 0.724 | 0.471 |
| DBP-3 | 82.42 ± 7.877 | 78.70 ± 10.066 | 2.058 | 0.042 |
| DBP-4 | 78.04 ± 6.509 | 78.26 ± 8.238 | -0.148 | 0.883 |
| DBP-5 | 77.26 ± 7.376 | 77.52 ± 8.190 | -0.167 | 0.868 |
| DBP-6 | 77.10 ± 5.068 | 77.54 ± 6.575 | -0.375 | 0.709 |
| DBP-7 | 76.04 ± 6.803 | 78.02 ± 6.832 | -1.452 | 0.150 |
| DBP-8 | 77.04 ± 6.518 | 76.60 ± 8.236 | 0.296 | 0.768 |
| DBP-9 | 77.00 ± 8.303 | 76.74 ± 7.491 | 0.164 | 0.870 |
| DBP-10 | 76.80 ± 6.007 | 76.96 ± 7.295 | -0.120 | 0.905 |
| DBP-11 | 76.72 ± 5.782 | 76.16 ± 7.875 | 0.405 | 0.686 |
| DBP-12 | 76.30 ± 7.080 | 76.16 ± 7.427 | 0.096 | 0.923 |
Table 5 shows that there was significant difference between the VAS score from 5th postoperative hr to 12th hr except in the 6th hr. This statistical difference was due to lower VAS score in Group-R.
Table 5: VAS distribution in two groups
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| VAS-Immediate postoperative period | 22.20 ± 5.067 | 23.20 ± 8.676 | -.704 | 0.483 |
| VAS-1 | 29.20 ± 4.445 | 27.40 ± 5.997 | 1.705 | 0.091 |
| VAS-2 | 30.96 ± 8.002 | 28.80 ± 8.722 | 1.290 | 0.200 |
| VAS-3 | 28.60 ± 9.260 | 26.60 ± 7.174 | 1.207 | 0.230 |
| VAS-4 | 28.60 ± 4.953 | 27.40 ± 4.870 | 1.222 | 0.225 |
| VAS-5 | 31.00 ± 4.629 | 27.80 ± 4.647 | 3.450 | 0.001 |
| VAS-6 | 29.40 ± 4.243 | 27.80 ± 5.067 | 1.712 | 0.090 |
| VAS-7 | 30.00 ± 2.020 | 27.40 ± 4.870 | 3.487 | 0.001 |
| VAS-8 | 30.40 ± 3.476 | 26.80 ± 4.712 | 4.347 | <0.001 |
| VAS-9 | 30.80 ± 3.959 | 25.40 ± 5.789 | 5.445 | <0.001 |
| VAS-10 | 28.20 ± 3.881 | 23.40 ± 5.573 | 4.998 | <0.001 |
| VAS-11 | 23.60 ± 4.849 | 20.60 ± 4.243 | 3.293 | 0.001 |
| VAS-12 | 21.40 ± 4.522 | 16.20 ± 4.903 | 5.513 | <0.001 |
Table 6 shows that there was significant difference between these two groups in VRS score in immediate post-operative period, 1st hr, 3rd hr and then from 7th hr to 12th hr. This difference is due to the lower VRS score in Group-R.
Table 6: Verbal rating scale distribution
| VRS time | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| VRS-Immediate postoperative period | 1.92 ± .340 | 1.62 ± .567 | 3.205 | 0.002 |
| VRS-1 | 2.04 ± .283 | 1.74 ± .565 | 3.359 | 0.001 |
| VRS-2 | 2.08 ± .665 | 1.84 ± .817 | 1.611 | 0.110 |
| VRS-3 | 1.88 ± .799 | 1.52 ± .646 | 2.477 | 0.015 |
| VRS-4 | 1.82 ± .438 | 1.68 ± .471 | 1.540 | 0.127 |
| VRS-5 | 2.06 ± .424 | 1.96 ± .283 | 1.387 | 0.169 |
| VRS-6 | 1.94 ± .424 | 1.80 ± .495 | 1.519 | 0.132 |
| VRS-7 | 2.02 ± .247 | 1.78 ± .465 | 3.226 | 0.002 |
| VRS-8 | 1.90 ± .416 | 1.64 ± .485 | 2.876 | 0.005 |
| VRS-9 | 2.06 ± .373 | 1.56 ± .501 | 5.657 | <0.001 |
| VRS-10 | 1.58 ± .499 | 1.32 ± .471 | 2.680 | 0.009 |
| VRS-11 | 1.26 ± .443 | 1.00 ± .000 | 4.149 | <0.001 |
| VRS-12 | 1.10 ± .303 | 1.00 ± .000 | 2.333 | 0.022 |
The number of patients requiring rescue analgesia was comparable in both groups and was non-significant. There was a statistical difference between the groups at the 9th hour. Table 7)
Table 7: Number of patients requiring rescue analgesics
| Postoperative
time interval |
Group-B (n=50) | Group-R (n=50) | c2 | p-value | ||
| No. | % | No. | % | |||
| Immediate period | 1 | 2 | 0 | 0 | 1.010 | 0.315 |
| 1st hour | 5 | 10 | 3 | 6 | 0.543 | 0.461 |
| 2nd hour | 17 | 34 | 16 | 32 | 0.045 | 0.832 |
| 3rd hour | 22 | 44 | 13 | 26 | 3.560 | 0.059 |
| 4th hour | 3 | 6 | 2 | 4 | 0.211 | 0.646 |
| 5th hour | 4 | 8 | 1 | 2 | 1.895 | 0.169 |
| 6th hour | 1 | 2 | 2 | 4 | 0.344 | 0.558 |
| 7th hour | 1 | 2 | 1 | 2 | 0.000 | 1.000 |
| 8th hour | 1 | 2 | 0 | 0 | 1.010 | 0.315 |
| 9th hour | 7 | 14 | 0 | 0 | 7.527 | 0.006 |
| Total doses of rescue analgesia required | 60 | 38 | – | – | ||
The time required for rescue analgesia was less in bupivacaine group than with ropivacaine, which means Group-R has a longer action for relief of pain. Also the total analgesia required is with ropivacaine less but was statistically insignificant Table 8)
Table 8: Time to 1st analgesic requirement
| Variables | Group-B
(Mean ± SD) |
Group-R
(Mean ± SD) |
t-value | p-value |
| Time to 1st Analgesic Requirement | 117.55 ± 46.856 | 131.03 ± 33.795 | -1.429 | 0.157 |
| Total Analgesia Consumption (mg) | 97.34 ± 46.693 | 83.82 ± 24.528 | 1.540 | 0.128 |
DISCUSSION
In comparisons to open cholecystectomy, LC is associated with less intense pain.9,10,11
In the present study, heart rates were lower in Group-R than in Group-B and that too for a longer time probably due to more dense and prolonged analgesia. Incidence of bradycardia was significantly higher with ropivacaine compared to bupivacaine, which was statistically significant. Gupta et al did same study with fentanyl and bupivacaine but the incidence of bradycardia was not increased.8The reason for this difference in incidence between the two studies could not be ascertain
Blood pressures (systolic, diastolic, and mean) were comparable and statistically insignificant in both the study groups, the reason being the rescue analgesia given on demand whenever VAS scores reached 40. Studies done by Gupta et al, Tae Han Kim et al, Goldstein et al also revealed the same findings, moreover none of the agents used intraperitoneally were described as causing rise in blood pressure.8,13,14
Our study (Table 5) showed that the analgesic effect was more pronounced with ropivacaine in the 7th hr. The difference in VAS score increased from 7th hr similarly, VRS scores in Group-B and in Group-R were significantly reduced in the immediate postoperative period and at first hr respectively. At 3rd hour VRS scores showed significantly less pain in patients receiving ropivacaine. VRS scores at the end of 7th hour showed a significant difference with ropivacaine (2.02 ± 0.247 in Group-B and 1.78 ± 0.465 in Group-R).Therefore, VAS and VRS were more in Group-B than in Group-R at all-time intervals.
Refaie et al12 and Scheinin et al15 also concluded that intensity of pain is reduced with bupivacaine compared to normal saline. Pain scores were 1.7 ± 0.2, 1.2 ± 0.1 and 0.9 ± 0.2 with bupivacaine at one, two and three hrs respectively vs. 1.9 ± 0.2, 3.2 ± 0.2 and 1.3 ± 0.3 in group with saline.12
Kim TH et al also concluded that intraperitoneal instillation of ropivacaine at the beginning of LC combined with normal saline infusion is an effective method for reducing pain after LC.13 Newcomb et al conducted a study to compare the efficacy of local anesthetic infiltration with or without preoperative non-steroidal anti-inflammatory drugs.16 They concluded that the use of preoperative rofecoxib, 0.5% bupivacaine infiltration, or both for postoperative analgesia did not decrease post-operative pain or decrease length of stay after LC compared with placebo. However, in our study intraperitoneal instillation of both bupivacaine and ropivacaine reduced the pain.
In 2007, Kucuk et al determined the effect of local anesthetic instillation and compared bupivacaine and ropivacaine in patients undergoing LC. The study showed that intraperitoneal instillation of 100 mg bupivacaine, 100 mg ropivacaine, or 150 mg ropivacaine at the end of a LC significantly reduced the morphine consumption during the first 24 h. For preventing postoperative pain. 150mg ropivacaine proved to be significantly more effective than either 100 mg bupivacaine or 100 mg ropivacaine.2 Ropivacaine proved more useful than bupivacaine in reducing the intensity of pain up to 12 hrs.
The number of patient requiring analgesia was not significantly different between the two groups up to 8th hr, which implies the pain relief was comparable between the two groups. In the 9th hr there was a significant difference between the two groups and from 10th hr onwards no patient required analgesia in either group. The number of patients receiving bupivacaine required more frequent dosing of analgesics and up to later periods of monitoring in postoperative hours, whereas requirement of second dose of analgesia got decreased and interval between two doses got increased considerably in patient receiving ropivacaine. A study done by Ashraf et al showed that the total analgesia requirement for patients with bupivacaine was lesser than with patients given normal saline,17 whereas Kang H et al compared ropivacaine with normal saline and showed better analgesia with ropivacaine.13
Time to first analgesic requirement was shorter with bupivacaine. The total analgesic dose consumption was also higher in this group. The differences in time to first analgesic requirement and total analgesic consumption were statistically insignificant (p < 0.05). This implies that the analgesia provided by ropivacaine is of longer duration and denser than bupivacaine. Total dose of analgesic consumption was higher in our study groups as compared to Gupta et al; this was probably due to tramadol given in premedication and longer duration of surgery in their study. Multiple doses of fentanyl and denser analgesia and sedation could have further lead to subsequent lesser dosing. In 2007, a similar study was conducted by Kucuk et al which showed that the intraperitoneal instillation of 100 mg bupivacaine, 100 mg ropivacaine, or 150 mg ropivacaine at the end of a LC significantly reduced the morphine consumption during the first 24 hrs.2 The instillation of ropivacaine 150 mg was more effective than bupivacaine 100 mg or ropivacaine 100 mg. Trikoupi et al also recorded the time of the first analgesic demand; the total amount of morphine received through PCA in the first 24 hours, and revealed similar results to us.18
Goldstein et al recorded that morphine consumption at wake-up and over the first 24 hr was significantly lower with bupivacaine and ropivacaine when compared with normal saline.14A study done by Rafaei et al revealed that the number of patients who needed postoperative analgesia in with bupivacaine was significantly lower than control.12 The morphine sparing effect of ropivacaine was significantly greater than that of bupivacaine. Park et al used fentanyl as rescue analgesia and concluded that fentanyl dose consumption was less in ropivacaine than normal saline.20 Sarvestani et al conducted a study using hydrocortisone which resulted in decreased pain and analgesic requirement.19
Complications
Ten percent of patients in the bupivacaine group had intra-operative complications. Incidence of bradycardia was more in Group-R (18%) than in Group-B (2%), and difference was statistically significant (p = 0.008).
Incidence of hypotension was more in patients receiving ropivacaine (6%) than bupivacaine (0%) but the results were not statistically significant (p = 0.079).
Incidence of emesis was equal in both the groups.
Incidence of pruritus was more with ropivacaine (12%) than with bupivacaine (4%), but difference was statistically insignificant (p = 0.140). Pruritus was self-limited.
The incidence of shoulder pain was less in our study perhaps because postoperative follow up was of shorter duration.
Limitations of the study
Patients were followed for 12 hour postoperatively which might have led us to overestimate rescue analgesic dose, as after 12 hours intensity of pain is decreased and less number of analgesic doses are required. Duration of analgesia provided could have been ascertained more precisely if study would have been longer.
We compared 2 µg/kg of bupivacaine and 2 µg/kg of ropivacaine. Cardiotoxicity and central nervous side effects of ropivacaine are less compared to bupivacaine in same plasma concentration.5,21,22 but, absorption after intraperitoneal instillation may be rapid, leading to plasma concentrations above the central nervous system toxicity threshold. We did not measure the plasma concentration of either drug. During general anesthesia, signs of neurological toxicity are masked, which calls for caution in dosing.
CONCLUSION
The results of our study show that intraperitoneal instillation of local anesthetic solution in laparoscopic cholecystectomy provides effective postoperative analgesia, and analgesia provided by ropivacaine is of longer duration as compared to bupivacaine.
Conflict of interest: None declared by the authors
Authors’ contribution: RKM – concept of study and manuscript editing
KM – conduction of study and data collection
SL – statistical analysis and literature search
SP – manuscript editing
REFERENCES
- Cuschieri A. Laparoscopic cholecystectomy. J R Coll Surg Edinb. 1999 Jun;44(3):187-92. [PubMed]
- Kucuk C, Kadiogullari N, Canoler O, Savli S. A placebo-controlled comparison of bupivacaine and ropivacaine instillation for preventing postoperative pain after laparoscopic cholecystectomy. Surg Today. 2007;37(5):396-400. [PubMed]
- Narchi P, Benhamou D, Fernandez H. Intraperitoneal local anaesthetic for shoulder pain after day-case laparoscopy. Lancet. 1991 Dec 21-28;338(8782-8783):1569–70. [PubMed]
- Chundrigar T, Hedges AR, Morris R, Stamatakis JD. Intraperitoneal bupivacaine for effective pain relief after laparoscopic cholecystectomy. Ann R Coll Surg Engl. 1993 Nov;75(6):437–9. [PubMed] [Free full text]
- Boddy AP, Mehta S, Rhodes M. The effect of intraperitoneal local anesthesia in laparoscopic cholecystectomy: a systematic review and meta-analysis. Anesth Analg. 2006 Sep;103(3):682-8. [PubMed]
- Gupta A, Thorn SE, Axelsson K, Larsson LG, Agren G, Holmström B, et al. Postoperative pain relief using intermittent injections of 0.5% ropivacaine through a catheter after laparoscopic cholecystectomy. Anesth Analg. 2002 Aug;95(2):450-6. [PubMed]
- Trikoupi A, Papavramidis T, Kyurdzhieva E, Kesisoglou I, Vasilakos D. Intraperitoneal administration of ropivacaine during laparoscopic cholecystectomy: 14AP12-5. Eur J Anaesth. 2010;27 :(47) :222. [Free full text]
- Gupta R, Bogra J, Kothari N, Kohli M. Postoperative analgesia with intraperitoneal fentanyl and bupivacaine: A randomized control trial. Can J Med. 2010;1(Suppl 1):1–9.
- Bisgaard T, Klarskov B, Kristiansen VB, Callesen T,Schulze S, Kehlet H, et al. Multi‐regional local anaesthetic infiltration during laparoscopic cholecystectomy in patients receiving prophylactic multi‐modal analgesia: a randomized, double‐blinded, placebo‐controlled study. Anesth Analg. 1999 Oct;89(4):1017–24. [PubMed]
- Joris J, Thiry E, Paris P, Weerts J, Lamy M. Pain after laparoscopic cholecystectomy: characteristics and effect of intraperitoneal bupivacaine. Anaesth Analg. 1995 Aug;81(2):379-84. [PubMed]
- Hendolin HI, Pääkkönen ME, Alhava EM, Tarvainen R, Kemppinen T, Lahtinen P. Laparoscopic or open cholecystectomy:a prospective randomised trial to compare postoperative pain, pulmonary function, and stress response. Eur J Surg. 2000 May;166(5):394-9. DOI: 10.1080/110241500750008961. [PubMed]
- Rafaie AMN, Khatab MM. Reduction of early postoperative pain after diagnostic laparoscopy with local bupivacaine: a randomized placebo controlled study. J Middle East Fertility Society. 2005;10(3):244-49.
- Kim TH, Kang H, Park JS, Chang IT, Park SG. Intraperitoneal Ropivacaine Instillation for Postoperative Pain Relief after Laparoscopic Cholecystectomy. J Korean Surg Soc. 2010;79:130-136. [Free full text]
- Goldstein A, Grimault P, Henique A, Keller M, Fortin A, Darai E. Preventing postoperative pain by local anesthetic instillation after laparoscopic gynecologic surgery: a placebo-controlled comparison of bupivacaine and ropivacaine. Anesth Analg. 2000 Aug;91(2):403-7. [PubMed]
- Scheinin B, Kellokumpu I, Lindgren L, Haglund C, Rosenberg PH. Effect of intraperitoneal bupivacaine on pain after laparoscopic cholecystectomy. Acta Anaesthesiol Stand. 1995 Feb;39(2):195-8. [PubMed]
- Newcomb W, Lincourt A, Hope W, Schmelzer T, Sing R, Kercher K, et al. Prospective, double-blinded, randomized, placebo-controlled comparison of local anesthetic and nonsteroidal anti-inflammatory drugs for postoperative pain management after laparoscopic surgery. Am Surg. 2007 Jun;73(6):618-24; discussion 624-5. [PubMed]
- Readman E, Maher PJ, Ugoni AM, Gordon S. Intraperitoneal ropivacaine and a gas drain: Effects on postoperative pain in laparoscopic surgery. J Am Assoc Gynecol Laparosc. 2004;11:486–91. [PubMed]
- Louizos AA, Hadzilia SJ, Leandros E, Kouroukli IK, Georgiou LG, Bramis JP. Postoperative pain relief after laparoscopic cholecystectomy: A placebo-controlled double-blind randomized trial of preincisional infiltration and intraperitoneal instillation of levobupivacaine 0.25% Surg Endosc. 2005;19:1503–6. [PubMed]
- Sarvestani AS, Amini S, Kalhor M, Roshanravan R, Mohammadi M, Lebaschi AH. Intraperitoneal hydrocortisone for pain relief after laparoscopic cholecystectomy. Saudi J Anaesth. 2013 Jan;7(1):14-7. doi: 10.4103/1658-354X…[Pubmed] [Free full text]
- Park YH, Kang H, Woo YC, Park SG, Baek CW, Jung YH, et al. The effect of intraperitoneal ropivacaine on pain after laparoscopic colectomy: a prospective randomized controlled trial. J Surg Res. 2011 Nov;171(1):94-100. doi10.1016/j.jss.2010.03.024. [PubMed]
- Barczynski M, Konturek A, Herman RM. Superiority of preemptive analgesia with intraperitoneal instillation of bupivacaine before rather than after the creation of pneumoperitoneum for laparoscopic cholecystectomy: a randomized, double-blind, placebo controlled study. Surg Endosc. 2006 Jul;20(7):1088-93. [PubMed]
- Labaille T, Mazoit JX, Paqueron X, Franco D, Benhamou D. The clinical efficacy and pharmacokinetics of intraperitoneal ropivacaine for laparoscopic cholecystectomy. Anesth Analg. 2002 Jan;94(1):100- [PubMed]
- Knudsen K, Beckman Suurkula M, Blomberg S, Sjovall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997 May;78(5):507- [PubMed] [Free full text]
↧
↧
Risk factors for thoracic surgery
Muhammad Saqib, MBBS, MCPS, FCPS
Classified Anesthesiologist, Combined Military Hospital, Kohat Cantt (Pakistan)
Correspondence: Col Muhammad Saqib, Classified Anesthesiologist, Combined Military Hospital Kohat Cantt (Pakistan); Email: bandeshah65@yahoo.com
ABSTRACT
Thoracic anesthesia for non-cardiac surgery has become a subspecialty and has its own challenges of being proficient in new surgical techniques and equipment in the clinical practice. Risk factors for thoracic surgery numerous, and include generally poor health of the patient, obesity, smoking, alcohol abuse, tumors pressing airways or great vessels of chest and pneumonectomy. Intraoperatively requirements of lateral position, one lung anesthesia and expected hemorrhage are the main risk factors. Postoperatively, infection, hemorrhage, risk of pulmonary embolism, tension pneumothorax and blow out of stump may adversely affect the outcome. Good selection and preparation of patients for thoracic surgery is very important to avoid high morbidity and mortality. Main aim of a good thoracic anesthesia plan is to avoid hypoxia and cardiovascular morbidity in the perioperative period.
Key words: Anesthesia; Anesthesia Department: Epidural Anesthesia; Thoracic surgery; Risk Factors; Risk Assessment; Intubation, Intratracheal; Thoracostomy
Citation: Saqib M. Risk factors for thoracic surgery. Anaesth Pain & Intensive Care. 2016;20 Suppl 1;S77-S80
Received: 8 August 2016; Edited: 11 September, 10 October 2016; Accepted: 10 September 2016.
INTRODUCTION
Anesthesia for thoracic surgery has always been a big challenge for the anesthesiologist. A very comprehensive knowledge of respiratory anatomy and physiology is required for good thoracic anesthesia, as well as to deal with the complications arising during its delivery. Increased incidence of lung cancer and respiratory infections due to heavy environmental pollution has increased the non-cardiac thoracic surgery manyfold. Thoracic anesthesia presents a unique set of physiologic problems: lateral decubitus position, open pneumothorax and need of one lung ventilation. These physiologic changes require careful attention of the anesthesiologist to avoid serious complications.1
PREOPERATIVE EVALUATION
Preoperative evaluation should focus on the extent and severity of pulmonary disease and cardiovascular involvement. In the history details about dyspnea, cough, characteristics of sputum, cigarette smoking, exercise tolerance, and alcohol abuse should be obtained. Physical examination is done to find out any cyanosis, clubbing, obesity, posture of the patient during breathing and auscultation of the chest for any wheeze, wet sounds or murmurs. Patients have an increased risk when they are unable to climb two flights of stairs. Surgery for pulmonary malignancies needs specific assessment, taking into account the ‘four M’s’-mass effects, metabolic effects, metastases and medications.4
Laboratory studies that need to be done before thoracic surgery are electrocardiography, chest radiography, arterial blood gases, pulmonary function tests (FEV1, FEV1/FVC), CT, PET scan, diffusing capacity for carbon monoxide, maximal oxygen consumption and maximal stair climbing. A vital capacity of 50% below predicted or below 2 L is an indication of increased risk.5 The ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC) is useful in differentiating restrictive (normal ratio) from obstructive (low ratio) disease. A 15 % improvement in pulmonary function tests after bronchodilator therapy is an indication for continued preoperative therapy. A mass that is seen on computed tomography is more likely to be malignant if it also demonstrates enhanced glucose uptake on the positron emission tomography scan. Echocardiography is very useful to assess the cardiac function.
PREOPERATIVE MANAGEMENT
Prophylactic digitalis is required especially in resection of pulmonary tissues. Preoperative treatment of several conditions decreases postoperative complications.
Cessation of smoking at least 48 hours before surgery decreases carboxyhemoglobin but improvement in ciliary function and decrease in sputum production requires 8-12 weeks. Treatment of hypovolemia and electrolyte imbalance facilitates removal of bronchial secretions. Bronchodilatation may be achieved with sympathomimetic drugs, steroids, cromolyn sodium and/or parasympatholytic drugs. Treat pulmonary infection with antibiotics according to the results of the sputum culture and sensitivity tests. Morbid obesity may present a risk for airway management, positioning, difficulty in clearing secretions and chances of respiratory failure in postoperative period. Particular attention is required to avoid hypoxia in the perioperative and postoperative periods. When epidural catheter is considered to be placed it should be placed before induction of anesthesia to offer patient cooperation and decrease the incidence of neurological complications. At least 2 large IV cannulae (14-16 g) are mandatory. Central venous catheter, blood warmer, rapid infusion device are desired if blood loss is anticipated.
PEROPERATIVE MANAGEMENT
Induction of anesthesia and placement of the double lumen tube (DLT) may be hazardous in a patient with a tumor pressing the airway or superior vena cava. Spontaneous breathing and awake induction may be required in some patients with difficult airway or bronchopleural fistula. Left sided DLT is advantageous as compared to right sided DLT because of risk of collapse of right upper lobe. Flexible fiberoptic bronchoscope is very helpful in correct placement of the DLT. Slinger et al suggested routine use of flexible bronchoscope for correct placement of DLT to avoid critical complications.7 Avoiding high airway pressures while preventing hypoxemia during one lung anesthesia are very important to avert acute lung injury (ALI) in the postoperative period. Lateral position provides optimal access for most thoracic procedures. Unfortunately this position alters the normal ventilation /perfusion relationship (V/Q). These derangements are further accentuated by induction of anesthesia, muscle paralysis, opening the chest, surgical retraction and initiation of mechanical ventilation. Although perfusion continues to favor the lower lung, ventilation favors the upper lung. This mismatch markedly increases the risk of hypoxia. Also induction of general anesthesia decreases FRC and moves the lower lung (perfused) to a less compliant part of the compliance curve. Moreover, positive pressure ventilation favors the upper lung as it is more compliant. All these factors worsen V/Q mismatching and predispose to hypoxia. Due to open pneumothorax the lungs are kept expanded by the negative pleural pressure. When one side of the chest is opened the negative pleural pressure is lost and the lung is collapsed. Spontaneous ventilation with open pneumothorax in the lateral position results in paradoxical respiration and mediastinal shift. These two effects can cause progressive hypoxia and hypercapnia, but fortunately these can be overcome by the use of positive pressure ventilation. Intentional collapse of the lung on the operative side greatly facilitates most thoracic procedures but complicates anesthetic management. The collapsed lung continues to be perfused but is no longer ventilated. So the patient develops right to left intrapulmonary shunt and associated hypoxia. Mixing of oxygenated blood from the ventilated lung and unoxygenated blood from the collapsed lung widens alveolar to arterial gradient hypoxia. But fortunately the blood flow to the non-ventilated lung is decreased by hypoxic pulmonary vasoconstriction and surgical compression of the upper lung.
Techniques for one lung ventilation are use of double lumen endobronchial tube, single lumen endotracheal tube plus bronchial blocker and single lumen endobronchial tube. Double lumen endobronchial tube is often used for one lung anesthesia. Patient related indications for one lung ventilation are confining infection or bleeding to one lung and for separate lung ventilation for large cyst or bulla, bronchopleural fistula and tracheobronchial disruption. Procedure related indications are pneumonectomy, lobectomy, segmental resection, thoracoscopy, anterior approach to thoracic spine, esophageal surgery and bronchoalveolar lavage. The principle advantages of DLTs are relative ease of placement, the ability of ventilating, either one or both lungs, and the ability to suction either lung. Robert Shaw, Carlens and White DLTs are available. Carlens is for left side and White is for right side and these have carinal hooks. Most commonly used Robert Shaw DLTs are for both right and left sides and these are without carinal hooks. Placement of DLT is done with a curved blade laryngoscope. The DLT is passed with the distal curvature anterior after the tip enters the larynx, the tube is rotated 90 degrees to the side to be intubated. The tube is advanced till resistance is felt, the average length is about 29 cm at the teeth. The tube position is established using a preset protocol and confirmed by flexible fiberoptic bronchoscopy.7
Protocol for left sided DLT placement is that; inflate the tracheal cuff (5-10 ml) and check for bilateral breath sounds. Unilateral sounds indicate that the tube is too far, the tracheal lumen is endobronchial (withdraw the tube little up).Then inflate the bronchial cuff (1-2 ml) and clamp the tracheal lumen and check for left sided breath sounds. In case of persistence right sided breath sounds advance the tube. If there are unilateral right sided breath sounds, it is due to incorrect entry into right bronchus. Then selectively clamp each lumen and confirm one-lung ventilation. After clamping of tracheal lumen tidal volume is usually set to 10 ml/kg and the respiratory rate is increased by 20% to maintain minute volume and PCO2. Complications of DLT are hypoxia due to tube malplacement or occlusion, traumatic laryngitis and tracheobronchial rupture due to overinflation of the bronchial cuff. Besides routine monitors (ECG, EtCO2, SpO2, NIBP), direct arterial monitoring is indicated in patients with poor cardiac or respiratory reserve and in resection of large tumors. Serial arterial blood gases are very useful to confirm the adequacy of ventilation and oxygenation. During thoracotomy, a radial artery catheter is placed in the dependent arm to aid in stabilizing the catheter. Central venous pressure monitoring is highly advisable and it reflects the net effect of venous capacitance, blood volume, and right ventricular function. Pulmonary artery catheter and transesophageal echocardiography are indicated in left ventricle dysfunction. Premedication with a parasympatholytic agent is useful in drying airway secretions but avoid narcotics and benzodiazepines in labile patients. Induction and maintenance of anesthesia may be done with IV propofol, ketamine, succinylcholine, opioids, benzodiazepines, lignocaine and non-depolarizing muscle relaxants.
Zeldin et al pointed out factors leading to postpneumonectomy pulmonary edema in the postoperative period in their retrospective study.2 Licker et al found out 3% incidence of ALI in postpneumonectomy cases and pointed out four factors responsible for it : excessive intravascular volume, pneumonectomy, high intraoperative ventilatory pressures, and preoperative alcohol abuse.3 Considering these studies we need a very close monitoring of the ventilatory pressures to avoid damage to the ventilated dependent lung. Cardiovascular stability is to be maintained while avoiding intravascular overload. A central venous and intra-arterial line may be very helpful in monitoring the cardiovascular system. Colloids and blood products may be preferred over crystalloids to replace the ongoing losses. Nitrous oxide is not used in thoracic anesthesia to avoid expansion of closed space lesions like bullae and pneumothorax. But prolonged use of 100% oxygen may cause damage to the lung. A mixture of oxygen and medical air may be used to avoid this complication in cases requiring prolonged anesthesia. All the current anesthetic techniques have been used successfully for thoracic surgery but the combination of a potent halogenated agent and opioid is usually preferred.
The greatest risk of one lung ventilation is hypoxemia. To reduce this risk, the period of one lung and use 100% O2 ventilation may be kept to minimum. Hypoxemia during one lung ventilation may require one or more of the following measures: Periodic inflation of the collapsed lung,2 CPAP 5-10 cmH2O to the collapsed lung and early ligation of the ipsilateral pulmonary artery in pneumonectomy. Other measures like 5- 10 cmH2O PEEP to the ventilated lung, changing the tidal volume and the respiratory rate and continuous insufflation of O2 to the collapsed lung may improve hypoxemia. If hypoxia persists, immediately reexpand the collapsed lung and verify position of the tube. The ETT is suctioned to exclude excessive secretions or obstruction. Pneumothorax on the dependent ventilated side should be excluded.
POSTOPERATIVE MANAGEMENT
In the postoperative period most patients are extubated early to reduce the risk of pulmonary barotrauma, blowout of the bronchial stump and pulmonary infection. DLT is exchanged with regular tube. Patients are kept in PACU or ICU overnight at least. Ventilatory support may be required for fragile patients. Pain management in the postoperative period includes systemic opioids, patient controlled analgesia, NSAIDs, epidural analgesia, intercostal nerve blocks, intrapleural analgesia and cryoanalgesia. Other routine postoperative care includes semi-sitting position, supplemental O2 and close hemodynamic monitoring. Other procedures like mediastinoscopy, thoracoscopy, removal of mediastinal mass, esophageal and spine surgery require close monitoring and comprehensive postoperative care for successful outcome. Use of new surgical techniques like Harmonic scalpel and video–assisted thoracoscopic surgery has improved the outcome of thoracic surgery. Further, high skills are required in fiberoptic bronchoscopy and invasive cardiovascular monitoring to improve the anesthetic care of thoracic surgery patients.6
Conflict of interest: None declared by the author.
Author contribution: The author contributed in the literature search, data analysis and manuscript preparation, and accepts full responsibility for the material presented.
REFERENCES
- Raiten JM, Blank RS. Anesthetic Management of Post-Thoracotomy Complications. Principles and Practice of Anesthesia for Thoracic Surgery: Springer; 2011. p. 6018.
- Zeldin RA, Normandin D, Landtwing D, Peters RM. Postpneumonectomy pulmonary edema. J Thorac Cardiovasc Surg. 1984;87(3):359-65. [PubMed]
- Licker M, de Perrot M, Spiliopoulos A, Robert J, Diaper J, Chevalley C, et al. Risk factors for acute lung injury after thoracic surgery for lung cancer. Anesth Analg. 2003;97(6):1558-65. [PubMed] [Free full text] doi: 10.1213/01.ANE.0000087799.85495.8A
- Slinger P, Darling G. Preanesthetic assessment for thoracic surgery. Principles and Practice of Anesthesia for Thoracic Surgery: Springer; 2011. p. 11-34.
- Naithani U, Bajaj P, Bhatnagar N, Prasad CN. One year prospective analysis of morbidity and mortality associated with thoracic surgery. Anaesth Pain & Intensive Care. 2011;15(2):86-92. [Free full text]
- Campos JH. Update on tracheobronchial anatomy and flexible fiberoptic bronchoscopy in thoracic anesthesia. Curr Opin Anaesthesiol. 2009;22(1):4-10. [PubMed] doi: 10.1097/ACO.0b013e32831a43ab.
- Slinger PD. Fiberoptic bronchoscopic positioning of double-lumen tubes. J Cardiothorac Anesth. 1989;3(4):486-96. [PubMed]
↧
Early extubation in adult and pediatric open heart surgery; an experience from a tertiary care hospital of a developing country
Mohammad Irfan Akhtar1, Mohammad Hamid2
1Assistant Professor, Department of Anesthesia, Aga Khan University, Stadium Road, Karachi 74800, (Pakistan)
2Associate Professor, Department of Cardiac Anesthesia, Aga Khan University, Stadium Road, Karachi 74800, (Pakistan)
Correspondence: Dr Mohammad Irfan Akhtar, Assistant Professor, Department of Anesthesia, Aga Khan University, Stadium Road, Box 3500, Karachi 74800, (Pakistan); Phone: +92 3486 4637; E-mail: mohammad.irfan@aku.edu
Abstract
Numerous remarkable advances have been made in the perioperative care of both adults and children undergoing cardiac surgery. Improvements in the technology of CPB, advances in the techniques of surgery, a better understanding of the pathophysiology of the postoperative period, and refinements in anesthetic and ICU care have led to changes in the perioperative management of these patients. These changes have resulted in improved outcomes and shortened hospital stay. Fast track strategy (FTS) is one of the major advances in the sub-specialty of cardiac anesthesia practice. FTS is applicable to all moderate to low risk elective open heart adult and pediatric surgeries. The role of anesthesiologist in Fast Track extubation (FTE) is very crucial and decisive as perioperative physician. Teamwork in FTE execution is very important. Every team member should respect the opinion of other team member provided the opinion is in the best interest of the patient. Multiple studies conducted as clinical audits and case series to validate the safety and feasibility of fast track extubation in adult and pediatric open heart surgical patients at our institution. Fast track extubation was practically evolved at our institution in 2007. FTE cannot be predicted in all the cases as it depends upon intra-operative and post-operative course. Safety is the priority in the decision about fast track extubation.
Key words: Early Extubation; Open Heart Surgery; Tertiary care hospital; Adult;
Pediatric
Citation: Akhtar MI, Hamid M. Early extubation in adult and pediatric open heart surgery; an experience from a tertiary care hospital of a developing country. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S81-S85
Received: 17 May 2016; Reviewed: 10 August 2016; Corrected: 28 August 2016; Accepted: 16 September 2016
INTRODUCTION
Numerous remarkable advances have been made recently, both in the adult and pediatric cardiac surgery. Improvements in Cardiopulmonary Bypass (CPB) machines and surgical techniques, a better understanding of the pathophysiology of disease, refinements in anesthetic techniques and Critical Care have led to better outcome and shortened hospital stay. Fast track strategy (FTS) is one of the major advances in the sub-specialty of cardiac anesthesia practice. FTS is applicable in all moderate to low risk elective open heart adult and pediatric surgery.
Fast tracking was first introduced in adult cardiac surgery as a response to growing economic pressure in the United States in 1977 by Ott and colleagues.1 Early extubation, early ambulation, cardiac rehabilitation and early discharge are the four components of Fast track strategy
Fast track extubation (FTE) is the foundation stone of Fast track strategy in cardiac surgery and FTE is now a standard of care practice in adult and pediatric open-heart surgery.
The advantages of early extubation have been validated and2 investigators3–5 have developed a clinical pathways for safe and efficient approach for these patients. The prime objective of most studies was to establish a quick uncomplicated recovery pathway with minimal burden on the Critical Care Units (ICU).4 Different study outcomes have been used to determine the success of these pathways. Most investigators have concentrated on ventilation time, length of ICU and hospital stay and postoperative complications as the main outcome measures to validate success of fast-track strategy.7,8
Fast track extubation is a very safe practice in pediatric CHD surgical patients belonging to RACHS-1 category 1, 2 and 3 and this has been proven by various national and international studies.9,13,14,15 Fast track and ultrafast track extubation after pediatric open-heart surgery does not affect cardiac function.9 This practice is safe and feasible if applied with multi-disciplinary approach.
Fast track extubation is practical in the scenario of developing countries with limited health care resources. The primary objectives of fast track extubation for developing countries is cost effectiveness, reduction in ventilator-associated complications, better utilization of limited resources and patients own and the family mental satisfaction. Patient’s relatives feel satisfied when they see their patient conscious, awake and without ventilator support.
Protocols are meant to address issues before they occur. Institution specific protocols should be implemented to standardize systematic plans for weaning patients and managing issues to facilitate early ICU and hospital discharge. The protocols should involve all members of perioperative care team before implementation and should be tailored according to the situation for best patient centered outcome.
Protocols for Early Extubation in Open Heart Surgery:
Fast track extubation means extubation within 4-8 hours of arrival in the Cardiac Intensive Care unit (CICU). An expeditious version of fast track extubation is ultra-fast track or on table extubation being executed in the operating room (OR) shortly after end of surgery especially in pediatric CHD surgical patients.
Fast track extubation is made possible due to choice of better anesthetic techniques using short acting anesthetic medications, better surgical techniques with improved efficiency, and better perfusion techniques with less inflammatory response supplemented by myocardial protection. Trans Esophageal Echocardiography (TEE) is used to confirm accuracy of surgical correction. Improved post-operative multidisciplinary ICU care with better objective and subjective monitoring is also used.
The role of anesthesiologist in FTE is crucial and decisive as a perioperative physician. It pivots around the decision regarding selection of premedication, intra-operative anesthetic agents, post-operative analgesia, strategy and pharmacological intervention to reduce or avoid post-operative nausea and vomiting.
Protocols are based upon certain selection criteria in which moderate to low risk open-heart surgery patients are included after pre-operative anesthetic assessment. Goal oriented pre-operative assessment is an important factor in the selection of correct patients in which fast track extubation is applicable. The general inclusion criteria for adult fast track extubation being followed are patients undergoing elective open heart surgery, between the ages of 18 -75 years with mild (40-50% ejection fraction) to moderate (EF 30-40%) left ventricular (LV) dysfunction. Exclusion criteria are patients with severe LV dysfunction (EF < 30%, pre-operative Intra-aortic balloon pump (IABP) and dialysis dependent renal failure.
Communication with all the team members including CICU staff and intensivist has been emphasized. A communication form of the open heart surgery patient is sent to the CICU with detailed information about demographics, diagnosis, procedure, the tentative plan about the post-operative care mentioning ventilatory settings, monitoring, inotropes and fast track or conventional extubation. This pre-emptive communication is meant to make the CICU nursing staff prepared to address potential issues.
Fast track anesthesia constitutes anesthesia induction using low doses of fentanyl (3-8 μg/kg), propofol (1-2 mg/kg), and rocuronium (0.5-1 mg/kg). Anesthesia is maintained by using isoflurane (1 minimum alveolar concentration), with propofol infusion during Cardiopulmonary Bypass (CPB) at a rate of 2 mg/kg/hr. Bispectral index monitoring (BIS) is also utilized in patients to titrate the depth of anesthesia. After CPB, recruitment maneuvers are used to prevent atelectasis. Warming devices are part of the plan to prevent hypothermia. Following closure of sternum, the anesthetic depth is reduced to allow the patient to initiate ventilation and then weaned to a pressure-assist mode before transfer to CICU. In the CICU, the patient is rewarmed to a temperature of 36 0 C with assistance of warming blanket. He/she is assessed for chest tube output, arterial blood gases ABGs and hemodynamic parameters for two hours in order to make a decision regarding weaning from ventilator. After two hours of post-operative assessment weaning is initiated if the patients fulfills the weaning criteria. Patient ventilatory support is reduced under guidance of ABGs and biochemical status. Sedation is terminated after the patient initiates spontaneous breathing in addition to SIMV breaths. Weaning steps followed are reduction in FIO2 to 0.4, lowering PEEP if > 5 cm, decreasing SIMV to switch to spontaneous mode, decreasing pressure support (PS) to 8-10 cm/H2O and monitoring Rapid Shallow Breathing Index (RSBI).
Extubation criteria are based upon full Glasgow Coma Score (GCS), ability to cough and clear secretions, no airway edema, chest tube output < 100 ml/hr for two consecutive hours, stable hemodynamic parameters and normal oxygenation/and ventilation.
In pediatric open-heart surgical patients, chest tube output should be less than 2 ml/kg/hr for two consecutive hours and patients are rewarmed to 36○ C to allow weaning from elective positive pressure ventilation.
In pediatric patients planned for on table extubation with team decision, muscle relaxation is stopped at the end of chest wiring, analgesia optimized with IV paracetamol and chest wound is infiltrated with local anesthetic solution. Anesthesia is terminated after skin closure and dressing. The patient is put on spontaneous breathing, muscle relaxation is reversed after assessment with twitch monitor (with Train of four ratio > 0.9).12 The patient is then extubated after fulfilling the standard extubation criteria12 shifted to CICU with supplemental oxygen , invasive arterial line, and CVP monitoring in addition to standard non-invasive American Society of Anesthesiology (ASA) monitoring.
In 1990s, due to increased demands for cardiac surgery and high healthcare costs, physicians were pressurized to reduce resource consumption and attention was focused on decreasing the length of CICU stay. Several institutions began to manage selected cardiac surgery patients in a specialized recovery unit in order to prevent ICU stay altogether. In several institutions specialized units called Enhanced Step-Down or PACUs with trained nurses are available who are trained in focused FTE.10 The patients planned for FTS are transferred there with an aim of shifting to a regular nursing unit as soon as possible. Some investigators have even implemented ambulatory cardiac surgery programs for low risk open-heart surgery.
Teamwork in Fast Track extubation execution is very important. Every team member should respect the opinion of other team member provided the opinion is in the best interest of the patient care and outcome. Each team should know their domain, decided with mutual understanding. Any input, should be informed input, this is important for mutual trust and positive outcomes.
OUR EXPERIENCE OF FTE
Multiple clinical audits and case series have validated the safety and feasibility of fast track extubation in adult and pediatric open-heart surgical patients at our institution the Aga Khan University Hospital. Fast track extubation was practically evolved at our hospital in 2007. A prospective observational study was done to assess the success and failure of fast track extubation in elective CABG adult surgical patients and to look for the reasons of delayed extubation.11 All elective CABG surgery patients, with EF > 40 percent were included. Patients with IABP, chronic renal failure, respiratory compromise and on high inotropic support were excluded from this audit. Six hundred and fourteen patients underwent CABG surgery during the audit period, out of which 388 (63.19%) were planned for FTE. A total of 196 (49.5%) patients could be extubated within six hours of arrival in the cardiac ICU. Common reasons for delayed extubation were deep sedation in 46.5%, confusion 25%, excessive bleeding in 11.3% and high inotropic support in 5.68%. Major contributing factors for delayed extubation were identified in this audit and specific strategies were put in place for modifications in intra operative management.
Another prospective observational study with the objective of determining the safety profile of fast track extubation practice in terms of its success and reasons for its failure in adult open-heart surgical patients was conducted at our institution.12 Primary outcome measures in the selected patients were time of extubation, re-intubation within 24 hours of extubation and total ICU stay. A total of 290 adult elective cardiac surgery patients undergoing isolated CABG, isolated valve replacements, combined procedures and aortic root replacements were enrolled. A standardized anesthetic technique was adopted. Surgical and bypass techniques were tailored according to the procedure. Overall success rate of fast track extubation practice (extubation within 6 hours) was 51.9% Major reasons for failed fast track extubation were hemodynamic instability, drowsiness and bleeding. Re-intubation rate was 0.68 %. Average duration of CICU stay was significantly higher (51.9±17.03 hours) in cases that were extubated after 6 hours in comparison with fast track patients in which the ICU stay was 41.02±10.9 hours (P value = 0.0005). This study again reinforced the safety of fast track extubation. It was concluded that to implement the practice in its full capacity and benefit, a fast track protocol needed to be devised to standardize the practice.
Another study in our institution was conducted in Pediatric CHD surgery patients to assess the safety profile of FTE. This was a prospective observational study.13 A total of 71 pediatric patients (6 months to 18 years) were enrolled in the study. Standardized technique was employed and the same surgeon performed surgery on all patients. Surgical procedures included VSD closures 25(35.2%), Tetralogy total corrections 17 (23.9%), 14 (19.7%) ASD closures, Glenn shunts 4 (5.6%) and BT shunts 4 (5.6%). In twenty six patients (36.62%) the trachea was extubated in the operating room, 29 (40.85%) were extubated within 6 h of arrival in CICU. We were unable to extubate 16 (22.54%) patients due to multiple reasons. Overall success rate for fast track extubation was 77.47%. Main reasons for delayed extubation were excessive bleeding in 5 (31.3%) cases, hemodynamic instability in 4 (25%) cases and respiratory complication in 2 (12.5%). There was no re-intubation in the FTE cases. On the basis of this audit, it was recommended to use FTE in selected pediatric CHD surgical patients using a multidisciplinary approach.
Another retrospective audit was done to assess the safety of ‘on table examination’ after open heart surgery in children with the primary objective of assessment of the rate of postoperative complications.14 All pediatric congenital heart surgery patients who underwent open-heart surgery between January 2011 and June 2013 were included. Incidence of immediate postoperative complications including re-intubation, significant bleeding, low cardiac output syndrome, and arrhythmias in PICU were analyzed. Surgeries included: ventricular septal defect (47%, n = 39), followed by atrial septal defect (36%, n = 30), and TOF (15%, n = 12). Cardiopulmonary bypass and aortic cross clamp time were 72.3 ± 34.2 and 47.3 ± 27.8 minutes, respectively. The mean inotrope score was 2.66 ± 3.53. There was no mortality in the cohort, whereas 97.8% (n = 80) had no complications during PICU stay. One patient (1.1%) required re-intubation for respiratory failure and one patient (1.1%) had arrhythmia that was medically managed. The mean length of PICU stay was 1.77 ± 0.985 days. As a result of this audit it was concluded that On-table extubation in children after open-heart surgery was feasible and safe in selected group of patients. No major complications were observed in the PICU.
After the success of fast track extubation in pediatric CHD surgical patients, feasibility and safety of on table extubation was assessed in TOF total correction surgical patients. For several years it was standard practice to electively ventilate these patients in the post-operative period, but a paradigm shift is taking place towards early extubation in these patients. This is due to advancement and understanding of the negative impact of positive pressure ventilation in patients with right ventricular dysfunction, . A case series was documented to determine the safety and feasibility of OTE in elective TOF total correction cardiac surgical patients with an integrated team approach.15 A total of eight elective TOF patients were included in the series. Standardize anesthetic, surgical and perfusion techniques were used. All patients were extubated in the operating room safely. Apart from better surgical and bypass techniques, the most important factor leading to successful OTE was excellent analgesia. On the basis of the case series results, it was suggested to extubate selected TOF cardiac surgery repair patients on table safely with integrated multidisciplinary approach.
CONCLUSION
FTS is teamwork based upon anesthetic technique, surgical expertise, perfusion optimization and postoperative nursing care. Each component is very important and complements each other. Success is dependent upon careful selection of the correct patients, follow them intra-operatively and decide postoperatively about the safety and feasibility of FTE/OTE execution on the basis of objective criteria. FTE cannot be predicted for sure. It depends upon intra-operative and post-operative course. Safety is the priority in the decision about fast track extubation.
Conflict of interest: None
Authors’ contribution: Both author took equal part in the concept, data search and manuscript preparation and reviewing
REFERENCES
- Ott RA, Gutfinger DE, Miller MP, Selvan A, Codini MA, Alimadadian H, et al. Coronary artery bypass grafting “on pump”: role of three-day discharge. Ann Thorac Surg. 1997;64(2):478-81. [PubMed] [Free full text] doi: 10.1016/S0003-4975(97)00542-0
- Cheng DCH, Karski J, Peniston C, Raveendran G, Asokumar B, Carroll J, et al. Early Tracheal Extubation after Coronary Artery Bypass Graft Surgery Reduces Costs and Improves Resource UseA Prospective, Randomized, Controlled Trial. Anesthesiology. 1996;85(6):1300-10. [PubMed] [Free full text]
- Engelman RM, Rousou JA, Flack JE, Deaton DW, Humphrey CB, Ellison LH, et al. Fast-track recovery of the coronary bypass patient. Ann Thorac Surg. 1994;58(6):1742-6. [PubMed]
- Cheng DCH, Karski J, Peniston C, Asokumar B, Raveendran G, Carroll J, et al. Morbidity outcome in early versus conventional tracheal extubation after coronary artery bypass grafting: a prospective randomized controlled trial. J Thorac Cardiovasc Surg. 1996;112(3):755-64. [PubMed] [Free full text] DOI: 10.1016/S0022-5223(96)70062-4
- Myles PS, Daly DJ, Djaiani G, Lee A, Cheng DCH. A systematic review of the safety and effectiveness of fast-track cardiac anesthesia. Anesthesiology. 2003;99(4):982-7. [PubMed] [Free full text]
- Paone G, Higgins RS, Havstad SL, Silverman NA. Does age limit the effectiveness of clinical pathways after coronary artery bypass graft surgery? Circulation. 1998;98(19 Suppl):II41-5. [PubMed]
- Parlow JL, Ahn R, Milne B. Obesity is a risk factor for failure of fast-track extubation following coronary artery bypass surgery. Can J Anesth 2006; 53:288-94. [PubMed] [Free full text] doi: 10.1007/BF03022217
- Ahonen J, Olkkola KT, Verkkala K, Heikkinen L, Seppala T, Ikavalko H, et al. Comparison of alfentanil, fentanyl and sufentanil for total intravenous anesthesia with propofol in patients undergoing coronary artery bypass surgery. Br J Anesth 2000; 85:533-40. [PubMed] [Free full text] doi: 10.1093/bja/85.4.533
- Meissner U, Scharf J, Dötsch J, Schroth M. Very early extubation after open-heart surgery in children does not influence cardiac function. Pediatr Cardiol. 2008 Mar; 29(2): 317-20. [PubMed] [Free full text] doi: 10.1007/s00246-007-9023-0
- Probst S, Cech C, Haentschel D, Scholz M, Ender J. A specialized post anesthetic care unit improves fast-track management in cardiac surgery: a prospective randomized trial. Crit Care. 2014 Aug 15;18(4):468. [PubMed] [Free full text] doi: 10.1186/s13054-014-0468-2.
- Akhtar MI, Hamid M. Success and failure of fast track extubation in cardiac surgery patients of tertiary care hospital: one year audit. J Pak Med Assoc. 2009 Mar; 59(3):154-6. [Free full text]
- Akhtar MI, Hamid M,Sharif H,Samad K, Khan FH. Success and Failure Profile Of Fast Track Extubation In Adult Open Heart Surgery Patients of A Tertiary Care Hospital. Submitted for publication in JCPSP Ref: No 1713/OA/2016.
- Akhtar MI, Hamid M, Minai F, Wali AR. Safety profile of fast-track extubation in pediatric congenital heart disease surgery patients in a tertiary care hospital of a developing country: An observational prospective study. J Anesthesiol Clin Pharmacol. 2014;30(3):355. [PubMed] [Free full text] doi: 10.4103/0970-9185.137267.
- Hoda M, Haque A, Aijaz F, Akhtar MI, Rehmat A, Amanullah M, et al. On-Table Extubation after Open Heart Surgery In Children: An Experience From A Tertiary Care Hospital In A Developing Country. Congenit Heart Dis. 2016; 11:58-62. [PubMed] [Free full text] doi: 10.1111/chd.12277
- Akhtar MI, Hamid M; Anwar-Ul-Haq, Minai F, Rehman N. Feasibility And Safety Of On Table Extubation After Corrective Surgical Repair Of Tetralogy Of Fallot In A Developing Country. A Case Series. Ann Card Anesth 2015; 18:237-241. [PubMed] [Free full text] doi: 10.4103/0971-9784.154490
↧
Comparison of intranasal dexmedetomidine and oral midazolam as premedication for cardiac catheterization procedure in pediatric patients
Nagesh Jambure, MD, FCA1 and Amarja Sachin Nagre, MD, DM, FCA1
1MGM Medical College / MGM Medical Centre and Research Institute, Aurangabad, Maharashtra, (India)
Correspondence: Dr Nagesh Jambure, Flat 13, 5th Floor, SAI Heritage, Ulkanagari, Aurangabad, Maharashtra, (India); Phone: +9579571122; E-mail: drnagesh83@gmail.com
ABSTRACT
Objective: The aim of study is to evaluate the preoperative sedative effects of intranasal dexmedetomidine as compared to oral midazolam as preanesthetic medication in children undergoing cardiac catheterization for diagnostic and/or therapeutic procedure. We aimed to compare the effects of drug between two groups.
Design: Prospective, randomized, double-blind, controlled study.
Methodology: 61 pediatric patients of either sex between the ages 2-10 years were recruited for cardiac catheterization for diagnostic and/or therapeutic procedural sedation. Patients were randomly divided into two groups; 31 patients (Group D) received intranasal dexmedetomidine 2 μg/kg by mucosal atomiser spray and 30 patients (Group M) received oral midazolam 0.5 mg/kg. Behavior score, sedation score, separation score and vital signs were recorded before shifting the patient to cathlab and at induction of anesthesia. The results were analyzed statistically.
Results: The result in the study shows that, group D patients (2 μg/kg) has statistically significant faster onset of action, separation score, sedation score, behavior score at induction and at 15 and 30 minutes as compared to group M (0.5 mg/kg).
Conclusion: Transnasal dexmedetomidine has faster onset of action, separation score, sedation score, and behavior score than oral midazolam for cardiac cath procedures in pediatric patients.
Keywords: Intranasal; Dexmedetomidine; Midazolam; Pediatric;
Premedication; Preanesthetic Medication
Citation: Jambure N, Nagre AS. Comparison of Intranasal dexmedetomidine and oral midazolam as premedication for cardiac catheterization procedure in pediatric patients.
Received: 20 June 2016; Reviewed: 27 June, 16 August 2016; Corrected: 29 June, 5 September 2016; Accepted: 30 September 2016
INTRODUCTION
Stranger anxiety and fear of separation from parents is common in pediatric patients.1 Preanesthetic medication in children should aim at relieving the stress response with preservation of hemodynamic parameter, facilitate the induction of anesthesia without prolonging the recovery and to produce amnesia.2 Therefore, pediatric pain management is challenging and one of the hallmark of modern anesthesiology. Numerous premedicants have been used through various routes; each route having its own merits and demerits.
Dexmedetomidine is a highly selective α2-adrenoceptor agonist which is eight times more α2 to α1-receptor selective than clonidine (1620:1 versus 200:1).3 As an α2-adrenoceptor agonist, dexmedetomidine has both sedative and analgesic effects without respiratory depression.4 The α2-adrenoceptor agonists achieve sedative effect through α2-adrenoceptors in the locus ceruleus in central nervous system. In addition, the delivery has extended to extra vascular routes including oral, buccal, transdermal, intramuscular and intranasal administration.5,6,7 These favorable properties have encouraged its use for a wide range of clinical conditions such as an anesthetic adjunct, postoperative sedation and pediatric premedication.5 81.8% (72.6–92.1%) of the nasally delivered medication actually ends up in the blood stream. The relatively large and well vascularized surface of the nasopharyngeal mucosa results in rapid absorption of delivered drug. The brain and nasal mucosa has neural connection which delivers the drugs to central nervous system.8,9,10 High first-pass metabolism of drug can be avoided by nasal administration.11
Thus, we conducted a study to compare the effects of transnasal dexmedetomidine and oral midazolam as premedicant in children undergoing cardiac catheterization for diagnostic and/or therapeutic procedure.
METHODOLOGY
After obtaining the local ethics committee approval and written informed consent from parents, 61 patients of either sex selected, between the ages 2-10 years. We examined the sedative and analgesic efficacy of intranasal dexmedetomidine and oral midazolam, in children undergoing cardiac catheterization for diagnostic and/or therapeutic procedural sedation like ASD device closure, VSD device closure, PDA device closure, balloon dilatation of aortic and pulmonary valve or cath angiography to decide operability of patient for surgical procedure. All patients were kept nil by mouth before the procedure. The oral group received midazolam 0.5 mg ̷ kg oral formulation and the intranasal group received dexmedetomidine 2µg ̷ kg diluted with 1 ml of distilled water, 0.5 ml in each nostril, by mucosal drug atomiser in the supine position. Patient with known allergy, oral and nasal deformity, mental retardation, A-V block, hepatorenal dysfunction, severe pulmonary hypertension, heart failure were excluded from study.
Patient were kept in cath lab recovery and connected to standard monitors. Baseline heart rate (HR), blood pressure (BP) and oxygen saturation (SpO2) were measured before premedication and Readings were taken at 15-min intervals up to 60 min, until child was separated from the parents. Premedication was given approximately 60min before induction of anesthesia. After the transnasal dose, sedation status was evaluated with 6-point score scale, and Behavior score and the ease of separation score were assessed with 4-point score scale by the blind observer.5 Mode of procedural IV sedation was decided by the attending anesthesiologist. A satisfactory sedation scores were considered in between 1 and 4 and unsatisfactory when rated 5 or 6. Children with scores of 1 or 2 were considered as a satisfactory behavior and separation scores and considered as unsatisfactory when behavior and separation scores were 3 or 4. The onset of action is defined as the time from the administration of the drug to the beginning of drowsiness. Children were also observed constantly for any side effect like nausea, vomiting, pruritus.
When procedure was finished, the child was placed in the recovery position and allowed to wake up naturally in the post cath ward. The time to achieve Aldrete score of 10, to be discharged from cath lab recovery, was recorded when child was awake, with vital signs within 20% of baseline values.
Statistical Analysis: Statistical analysis was done with the help of SPSS software. Sample size of 61 patients was calculated to be enrolled in the study. Quantitative data were presented with the help of mean and standard deviation. Comparison among study groups was done with the help of unpaired T-test. Levene’s test was used for equality of variances and t-test for equality of means. P value < 0.05 was taken as a level of significance.
Table 1: Evaluation scales
| Sedation score
1. Does not respond to mild prodding or shaking 2. Responds only mild prodding or shaking 3. Responds only after name is called loudly or repeatedly 4. Lethargic response to name spoken in normal tone 5. Appear asleep but respond readily to name spoken in normal tone 6. Appear alert and awake, response readily to name spoken in normal tone |
| Behavior scores
1. Calm and cooperative 2. Anxious but reassurable 3. Anxious and not reassurable 4. Crying, or resisting |
| Separation score
1. Patient unafraid, cooperative, asleep Excellent 2. Slight fear or crying, quite with reassurance 3. Moderate fear, crying not quite with reassurance 4. Crying need for restraint |
Result
Both the groups were comparable with regard to age and weight. In the present study, we assessed the onset, sedation, behavior, separation score and hemodynamic using the evaluation scale (Table 1). Three patient resisted intranasal drug administration were also included in study.
Table 2: Demographic profile
| Variable | Group D
(N=31) |
Group M
(N=30) |
P Value |
| Male* | 27(87.1%) | 19(63.3%) | 0.06 |
| Female* | 4(12.1%) | 11(36.7%) | 0.06 |
| Age (Years)** | 6.16 ± 2.37 | 5.83 ± 2.77 | 0.62 |
| Weight (kg)** | 17.58 ± 6.69 | 19.07 ± 6.76 | 0.391 |
*N(%); **mean ± SD
Comparison of demographic profile of patients in groups, shows that mean age was 6.16 ± 2.37 yr and 5.83 ± 2.77 yr in group D and group M respectively. Mean weight was 17.58 ± 6.69 kg and 19.07 ± 6.76 kg in two groups respectively which is comparable and not significant.
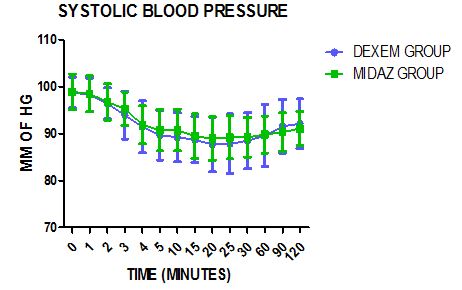
Figure 1: Systolic blood pressure

Figure 2: Diastolic blood pressure

Figure 3: Pulse rate
Figures 1, 2 and 3 show the comparison of preoperative vital signs in midazolam group and dexmedetomidine group. It suggest that mean systolic blood pressure, diastolic blood pressure and pulse rate are comparable and the difference is not statistically significant. The vital signs remained stable and comparable in both the groups throughout 120 min.
Table 3: Comparative analysis of sedation data in two groups (Mean ± SD, P < 0.05 Significant)
| Parameter | Group D
(N=31) |
Group M
(N=30) |
P Value |
| Onset of Action | 20.3 ± 4.39 | 27.03 ± 3.39 | .000 |
| Sedation Score Induction | 3.03 ± 0.48 | 4.03 ± 0.41 | .000 |
| Sedation Score 15 | 4.52 ± 0.68 | 5.4 ± 0.56 | .000 |
| Sedation Score 30 | 2.29 ± 0.64 | 3.33 ± 0.66 | .000 |
| Behavior Score Induction | 2.1 ± 0.4 | 2.83 ± 0.38 | .000 |
| Behavior Score 15 | 2.58 ± 0.5 | 3.6 ± 0.49 | .000 |
| Behavior Score 30 | 1.58 ± 0.5 | 2,57 ± 0.50 | .000 |
| Separation Score | 1.58 ± 0.5 | 2.67 ± 0.48 | .000 |
| Aldrete score of 10 | 55.16 ± 9.68 | 57.17 ± 2.84 | 0.28 |
As shown in table no 3, mean time for onset of action was 20.3 ± 4.39 and 27.03 ± 3.39 in group D and group M respectively. It was found that difference was significant and the time of onset of action is faster in group D than group M. Sedation score and Behavior score at 15 min in group D is satisfactory while group M is unsatisfactory, and statically significant at 30 min and at induction in group D than group M. Separation scores is also satisfactory in intranasal group. Time to achieve Aldrete score of 10 (time to be discharged from cath lab recovery) was similar in both groups. There were no children had reduction of spo2 below 95%.Two children in the intranasal group had bradycardia, one had hypotension and one children of the oral group had bradycardia. None of the patients required any pharmacological intervention.
Discussion-
Premedication is commonly used in pediatric patients to relieve the separation anxiety, to improve patient comfort & to make the procedure smooth and efficient. Intranasal medication offers a truly “needleless” solution to drug delivery. This route is easy, convenient, painless, comfortable, and avoids destruction by hepatic first pass metabolism. Dexmedetomidine is colorless, odorless, does not cause mucosal stimulation, and it has very good sedative, anxiolytic, causing no respiratory depression making it suitable for intranasal administration.12,13 In comparison, midazolam causes respiratory depression, excessive sedation, delirium, prolonged recovery time and so on.
Drugs absorbed via the nasal mucosa riches the vascular plexus of the nose, which directly enter the circulation and it also absorbed through the olfactory mucosa into the CSF – giving rapid brain levels of the drug.14,15
Particle size 10-50 microns adheres best to the nasal mucosa. Smaller particles pass on to the lungs, larger particles form droplets and run-out of the nose. Broad 30 micron spray ensure excellent mucosal coverage,16 and hence results in better absorption.17
In our study, we found that 2 µg/kg dexmedetomidine had statistically significantly faster onset i.e. 20 minutes. Telon et al. also used 2 μg/kg intranasal dexmedetomidine, and they observed that dexmedetomidine was more effective than oral midazolam as a preoperative sedative and the onset of action was 15 minutes.18 Yuen et al shows that 1 μg/kg intranasal dexmedetomidine has onset of sedation of approximately 25 minutes.19
We observed that the intranasal group achieved a better sedation score and behavior score of 3 or more at 15 min, 30 min and at induction than oral midazolam group. The separation scale was lower and statistically significant in group D.
Yuen compare the effects intranasal dexmedetomidine (0.5 µg/kg and 1 µg/kg) with oral midazolam (0.5 mg/kg) as a premedication for minor surgery in 96 children of 2- 12 years old. The results showed that children were significantly more sedated with intranasal dexmedetomidine than oral midazolam. There were no differences in parental separation acceptance and behavior score at induction or wake-up behavior score. 5
Yuen et al. also studied 116 children between 1 and 8 years of age, who received an intranasal dexmedetomidine of either 1 µg/kg and/or 2 µg/kg as a premedication. They observed adequate sedation in 53% of the children in the lower dose group at the time of induction versus 66% in the higher dose group.12 Cimen and colleagues enrolled 62 children (2–6 years of age) scheduled to undergo minor elective surgery into a randomized, double-blind trial comparing buccal and intranasal dexmedetomidine as a pre-induction sedative; 1 µg/kg dose of dexmedetomidine was given in both groups, 45 minutes prior to anesthetic administration. Sedation scores were significantly higher in the intranasal group, beginning at the 10 minutes and continuing until the final assessment at 45 minutes. Ease of parental separation was considered satisfactory in 75.5% of the intranasal group, compared to only 16.2% of the buccal group.20
In the present study, there was a no statistically significant decrease in SBP, DBP and HR from baseline up to 60 min after the administration of intranasal dexmedetomidine and oral midazolam. There was no significant reduction in SpO2 below 95% in both groups.
CONCLUSION
Thus from the results of our study, it is concluded that premedication with intranasal dexmedetomidine had statistically significantly faster onset, and lower sedation, behavior and separation scores, compared to oral midazolam. Moreover, 2 µg/kg dose of intranasal dexmedetomidine has faster onset of action than 1 µg/kg.
Acknowledgement-
We thank Dr. Antony Jorge, DM (Cardiac anesthesia), Sri Jayadeva Institute of Cardiology, Bangalore, for his statistical assistance.
Conflict of interest: Nil declared.
Authors’ contribution: Both authors took equal part in conduct of study and manuscript preparation
REFERENCES
- Kossowsky J, Wilhelm FH, Roth WT, Schneider S. Separation anxiety disorder in children: disorder-specific responses to experimental separation from the mother. J Child Psychol Psychiatry. 2012;53(2):178–87. [PubMed] DOI:10.1111/j.1469-7610.2011.02465.x
- Morgan-Hughes JO,Bangham JA. Preinduction behaviour of children. 1990;45(6):427-35. [PubMed] DOI:10.1111/j.1365-2044.1990.tb14326.x
- Bhana N, Goa KL, McClellan KJ. Dexmedetomidine.Drugs. 2000;59(2):263–8. [PubMed]
- Tsifansky, Michael D, Schmitt, Carol G, Muñoz, Ricardo A. Dexmedetomidine: do we know enough?.Pediatr Crit Care Med. 2007;8(5):492-3. [PubMed] DOI:10.1097/01.PCC.0000269380.66845.21
- Yuen VM, Hui TW, Irwin MG, Yuen MK. A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial.Anesth Analg, 2008;106(6):1715-21. [PubMed] DOI:10.1213/ane.0b013e31816c8929
- Anttila M,Penttilä J, Helminen A, Vuorilehto L, Scheinin H. Bioavailability of dexmedetomidine after extravascular doses in healthy subjects. Br J Clin Pharmacol. 2003;56(6):691-3. [PubMed] DOI: 10.1046/j.1365-2125.2003.01944.x
- Kivisto KT, Kallio A, Neuvonen PJ. Pharmacokinetics and pharmacodynamics of transdermal dexmedetomidine. Eur J Clin Pharmacol. 1994;46(4):345-9. [PubMed] DOI:10.1007/BF00194403
- Illum L. Transport of drugs from the nasal cavity to the central nervous system. Eur J Pharm Sci. 2000;11(1):1-18. [PubMed]
- Mathison S, Nagilla R, Kompella UB. Nasal route for direct delivery of solutes to the central nervous system: fact or fiction? J Drug Target. 1998;5(6):415-41. [PubMed] DOI: 10.3109/10611869808997870
- Thorne RG, Frey WH 2nd. Delivery of neurotrophic factors to the central nervous system: pharmacokinetic considerations. Clin Pharmacokinet. 2001;40(12):907-46. [PubMed] DOI: 10.2165/00003088-200140120-00003
- Knoester PD, Jonker DM, Van Der Hoeven RT, Vermeij TA, Edelbroek PM, Brekelmans GJ, et al.Pharmacokinetics and pharmacodynamics of midazolam administered as a concentrated intranasal spray. A study in healthy volunteers. British Journal of Clinical Pharmacology. 2002;53(5):501-7. [PubMed]
- Yuen VM, Hui TW, Irwin MG, Yao TJ, Chan L, Wong GL, Shahnaz MH, et al. A randomised comparison of two intranasal dexmedetomidine doses for premedication in children. Anaesthesia. 2012 Nov;67(11):1210–6. [PubMed] DOI: 10.1111/j.1365-2044.2012.07309.x.
- Ghali AM, Mahfouz AK, Al-Bahrani M. Preanesthetic medication in children: a comparison of intranasal dexmedetomidine versus oral midazolam. Saudi J Anaesth. 2011;5(4):387–91. [PubMed] DOI: 10.4103/1658-354X.87268
- Walberg EJ, Wills RJ, Eckhert J. Plasma concentrations of midazolam in children following intranasal administration.Anaesthesiology. 1991;74(2):233–45. [PubMed]
- Rey E, Delaunay L, Pons G, Murat I, Richard MO, Saint-Maurice C et al. Pharmokinetics of midazolam in children – comparative study of intranasal and intravenous administration.Eur J Clin Pharm. 1991;41:355–7. [PubMed] DOI: 10.1007/BF00314967
- Holsti M, Dudley N, Schunk J, Adelgais K, Greenberg R, Olsen C, et al. Intranasal midazolam versus rectal diazepam for the home treatment of acute seizure in paediatric patients with epilepsy.Arch Pediatr Adolesc Med. 2010;164(8):747-53. [PubMed] DOI: 10.1001/archpediatrics.2010.130.
- Wolfe TR, Bernstone T. Intranasal drug delivery: an alternative to intravenous administration in selected emergency cases. J Emerg Nurs. 2004;30(2):141–7. [PubMed] [Free Full Text] DOI: 10.1016/j.jen.2004.01.006
- Talon MD, Woodson LC, Sherwood ER, Aarsland A, McRae L, Benham T. Intranasal dexmedetomidine premedication is comparable with midazolam in burn children undergoing reconstructive surgery. J Burn Care Res. 2009;30(4):599–605. [PubMed] doi: 10.1097/BCR.0b013e3181abff90
- Yuen VM, Hui TW, Irwin MG, Yao TJ,Wong GL,Yuen MK. Optimal timing for the administration of intranasal dexmedetomidine for premedication in children. Anesthesia. 2010;65(9):922–9. [PubMed] DOI: 10.1111/j.1365-2044.2010.06453.x
- Cimen ZS, Hanci A, Sivrikaya GU,Kilinc LT,Erol MK. Comparison of buccal and nasal dexmedetomidine premedication for pediatric patients. Pediatr Anesth. 2013;23(2):134–8. [PubMed] DOI: 10.1111/pan.12025
↧
↧
Hazards and limitation of perioperative transfusion: need to adopt blood transfusion guidelines
Samina Ismail, FCPS1
1Professor of Anesthesiology, Department of Anesthesiology, Aga Khan University Hospital, Karachi, (Pakistan)
Correspondence: Professor Samina Ismail, FCPS, Department of Anesthesiology, Aga Khan University Hospital, Stadium Road, Box 3500, Karachi 74800, (Pakistan); Phone: Tel: +92 34 86 4631E-mail: samina.ismail@aku.edu
ABSTRACT
Blood transfusion is an important component of perioperative management of patients and in many instances can be lifesaving. Anesthesiologists are an important member of the multidisciplinary team involved regularly in requesting and administering blood components to the patients. Therefore, it is essential that anesthesiologists are familiar with indications and appropriate use of blood components and also with limitation and adverse effects associated with its use. Numbers of international guidelines regarding transfusion are available; however, these guidelines require local translation into policies, protocols and practice in order to deliver care to the patient. Institutions need to identify their local barriers and resources available and consult from the evidence based international guidelines to develop their own guidelines on blood transfusion. However, it must be remembered that it is a multidisciplinary engagement involving blood bank, laboratory, operating room and clinical staff; therefore, it is a challenging task which demands coordinated team work to translate guidelines into safe patient care.
Key Words: Blood transfusion; Policies; Blood transfusion guidelines; Hazards of blood transfusion; Inappropriate blood transfusion; Patient blood management
Citation: Ismail S. Hazards and limitation of perioperative transfusion: need to adopt blood transfusion guidelines. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S86-S90
Received: 29 July 2016; Reviewed: 8August 2016; Corrected: 28 August 2016; Accepted: 6 September 2016
INTRODUCTION
Blood transfusion can be lifesaving and its usage remains high in the perioperative period particularly in trauma, obstetric and cardiovascular surgery. However, in recent years there is a greater awareness related to transfusion related complications, resulting in increased scrutiny of the use of allogenic transfusion by medical professionals.1 This has led to development of number of guidelines to improve transfusion practices.
This article will focus on rational use of blood in special relation to its utilization in Pakistan, indication and hazards of transfusion and international guidelines related to transfusion.
RATIONAL USE OF BLOOD PRODUCTS
Rational use of blood implies that right blood product is to be given to the patient only when needed and in the right amount.2 Appropriate use of blood has been shown to reduce the number of transfusion by 30%.3
Inappropriate rate of transfusion ranges from 18-57%.4-12 According to World Health Organization (WHO) estimates, about 1.2-1.5 million units of blood are being transfused every year in Pakistan, leading to a shortage of 40% in the availability of blood.13,14 Studies conducted in Pakistan have shown a higher rate of transfusion in public sector hospitals then private sector.15,16 In the public hospital, appropriate use of blood was 54.1% as compared to the private hospital where the appropriate use of blood products was 69.4%.15 In both public and private hospitals, clinicians were not using guidelines and there was no method of documentation or taking consent from the patients.15,16
In addition to inappropriate transfusion, many units of blood are routinely ordered and not utilized. This happens in situation where maximum surgical blood ordering schedule (MSBOS) is not implemented. MSBOS is evidence based estimates of average requirement in a particular procedure thus avoiding subjective anticipation of blood loss by clinicians and has shown 60% reduction of cost to the patient.17
HAZARDS AND LIMITATION OF TRANSFUSION
Transfusion of allogenic blood component is not without hazards and can lead to serious consequences and therefore requires careful consideration.18 Allogenic transfusion is associated with transfusion reactions and both infectious and non-infectious complications. Infectious complication is caused by blood borne pathogens which includes cytomegalovirus, Human Immunodeficiency Virus (HIV) , hepatitis virus including B, C and E virus, Creutzfeldt-Jakob disease (CJD) and now more recently Ebola and Zika virus. Non-infectious risk of transfusion includes transfusion related acute lung injury (TRALI) and transfusion associated graft versus host disease, however, they can be reduced through introduction of leucodepletion and careful donor selection.19
Some studies have identified risk of immunosuppression with earlier recurrence and lower survival rates in patients with breast, colorectal and prostate cancer who received blood transfusion in the perioperative period ,19,20 but other data have negated the association.21 Increase rates of postoperative infections have also been associated with perioperative transfusion.22-25
Besides the risk of complication and safety concerns, there is an issue of rising cost with shortages of specialized blood components.26,27 It is of paramount importance that the practice of blood transfusion is safe and based on current scientific evidence-based indications.
INDICATION OF BLOOD TRANSFUSION
The provision of readily available blood is not only lifesaving but has facilitated medical development by enabling number of complex surgical procedures which would not have been possible otherwise. The transfusion of red blood cells (RBC) and blood products like fresh frozen plasma (FFP), cryoprecipitate and platelets have the benefits to improve tissue oxygenation and control bleeding hence having potential of improving clinical outcomes.28 However, controlled studies have not been performed to determine the haemoglobin concentration at which RBC transfusion improves clinical outcomes.28
Scientific indication for perioperative blood transfusion should base on two principal assumptions:
- When a surgical patient is experiencing adverse outcome due to decreased oxygen carrying capacity.
- These adverse outcomes can be prevented by RBC transfusion by enhancing oxygen carrying capacity.
Tissue oxygenation is well maintained at a haematocrit of 18-25% in healthy, normovolemic patients.29,30 The heart does start releasing lactic acid until the haematocrit drops down to 15-20% and myocardial lactate flux is not affected until haemoglobin concentrations drops to 6 gm/dL.29-31 In acute blood loss, reduction in arterial oxygen content is prevented because of compensatory increase in cardiac output and heart failure usually does not occur until the haematocrit reaches 10%.32,33 Although, this compensatory increase in cardiac output in response to acute blood loss may be affected by several factors such as; left ventricular dysfunction and use of vasoactive medications (beta adrenergic or calcium channel blockade) requiring higher haemoglobin concentration for adequate oxygen delivery to tissues. Tolerance to acute blood loss is also affected by anesthetics, and some case reports have suggested that patients may tolerate lower haemoglobin under anesthesia due to reduction of oxygen consumption.34 Yet no prospective randomized controlled trials have been done to support this statement.
Decisions regarding perioperative transfusion require clinical judgement and should not be based on a single transfusion trigger that fails to consider important physiological and surgical factor that affects oxygenation of tissues.
PATIENT BLOOD MANAGEMENT
This is patient based approach which focuses on the optimization of three perioperative factors: investigating and treatment of perioperative anaemia; reduction of perioperative blood loss and optimization of patient specific physiological reserve of anaemia.35
Process of Transfusion: This needs to be defined properly in every institution in order to avoid administering the wrong blood type in error. The following guidance is for manual checking process at the bedside:35
- All patients must be wearing an identity wrist band with their full names, date of birth and hospital identification number, which needs to be checked with the identification on the blood components immediately before transfusion.
- The blood components in addition to patient identification need to be checked for blood group, donation number and expiry date and time.
- Visually check for leakage, discoloration and clots.
- Two people need to check and sign both on the form and blood component bag.
- The date and time of start and end of transfusion required to be documented.
Monitoring of patients after the start of transfusion: Patients must be monitored for adverse transfusion reaction like any signs of tachycardia, rash, breathlessness hypotension and fever, which mandates stopping the transfusion and communication with the laboratory.36 The immediate treatment of any transfusion reaction includes stopping any further transfusion and administration of antihistamines, steroids and use of adrenaline if it is life threatening .37
TRANSFUSION GUIDELINES
Anesthesiologist as part of team involved in the perioperative management of patients makes transfusion decisions and administers blood and blood components. In order to make the transfusion practice safe and to guide clinical practitioners, number of practice guidelines for blood component transfusion therapy have been issued; including a report by the American Society of Anesthesiologists task force on blood component therapy in 1996,28 guidelines produced by the British Committee for Standards in Haematology (BCSH),38 and National Institute for Health and Care Excellent (NICE) guidelines39, 11 including NICE guidelines for trauma.40
The most recent Association of Anesthetists of Great Britain and Ireland (AAGBI) guidelines for the use of blood components and their alternatives from 2016 bring together three previous AAGBI guidelines: blood component therapy 2005; red cell transfusion 2008; and massive hemorrhage 2010.41 These guidelines have focused on clinical indications, risk of transfusion, blood conservation and transfusion process. The recommendations of these guidelines are as follows: 41
- Preoperative hemoglobin level needs to be measured before major elective surgery.
- WHO defines anemia as Hb level < 13 g/L for men and < 12 g/L for women.
- According to AAGBI guidelines patients labeled anemic according to WHO definition needs to be investigated before elective surgery and non-urgent elective surgery other than caesarean section needs to defer.
- Patient needs to be informed about the possibility of blood transfusion in cases where transfusion is anticipated and this should be properly documented in patients’ file notes.
- In cases where the bleeding is not ongoing and large deficit needs not be corrected, patient should be evaluated for further need of transfusion after every unit of red blood cell transfused.
- When blood loss of more than 500 ml is anticipated provision of cell salvaged and use of tranexamic acid needs to be considered.
- In pediatric population blood products should be prescribed by volume and not by number of units.
- Massive blood transfusion protocol should be present in every institution, which should regularly be reviewed and audited.
- Every institution should have an emergency supply of group O blood and mechanism of provision of group specific blood within 15-20 minutes of receiving correctly labeled samples and information of the emergency requirement of blood.
- Preference should be given to transfusion of red blood cells and FPP over other intravenous fluids in case of major hemorrhage due to trauma and obstetric reasons.
- In situations where patients continue to bleed, transfusion of blood products needs be gauged by regular laboratory tests for coagulation; FFP needs to be transfused if INR > 1.5, cryoprecipitate if fibrinogen is < 1.5 gm/L and platelets if platelets count is < 75 x 109 /L.
CONCLUSION
To date number of international guidelines regarding transfusion is available. However, it must be remembered that these guidelines require local translation into policies, protocols and practice in order to deliver care to the patient. Therefore, local barriers need to be identified and policies should be made according to local circumstances but international guidelines need to be consulted and followed. Education and training on blood transfusion guidelines, patient blood management, transfusion process and management of massive hemorrhage is required at the time of induction of health care staff and also at regular basis to reinforce already existing knowledge and training. As it is multidisciplinary engagement involving blood bank, laboratory, operating room and clinical staff, it is challenging and will require coordinated team work to translate guidelines into safe patient care.
Conflict of interest: None declared by the author. The author certifies that the contents declared above are correct to the best of her knowledge
Author’s contribution: SI is the sole author of this manuscript.
REFERENCES
- REFERENCES
- Practice guidelines for blood component therapy: a report by the American Society of Anesthesiologists Task Force on Blood Component Therapy. Anesthesiology. 1996;84:732-47. [PubMed] [Free full text]
- Ma M, Eckert K, Ralley F, Chin-Yee I. A retrospective study evaluating single-unit red blood cell transfusions in reducing allogeneic blood exposure. Transfus Med. 2005; 15: 307-12. [PubMed] [Free full text] doi: 10.1111/j.0958-7578.2005.00592.x
- Sharma R. South East Asia faces severe shortage of safe blood. BMJ. 2000; 320: 1026. [PubMed] [Free full text] doi: 10.1136/bmj.320.7241.1026
- Clarke AM, Dorman T, Bell MJ: Blood loss and transfusion requirements in total joint arthroplasty. Ann R Coll Surg Engl. 1992; 74:360-3. [PubMed] [Free full text]
- Goodnough LT, Verbrugge D, Vizmeg K, Riddell J IV: Identifying elective orthopedic surgical patients transfused with amounts of blood in excess of need: The transfusion trigger revisited [published erratum appears in Transfusion. 1992; 32:838] Transfusion 1992; 32:648-53. doi: 10.1046/j.1537-2995.1992.32792391039.x
- Gianoutsos MP, Thompson JF, Storey DW, Kronenberg H: The rational use of homologous blood in elective surgery. Aust N Z J Surg 1992; 62:266-9. [PubMed] [Free full text] doi: 10.1111/j.1445-2197.1992.tb07553.x
- Hallissey MT, Crowson MC, Kiff RS, Kingston RD, Fielding JW: Blood transfusion: An overused resource in colorectal cancer surgery. Ann R Coll Surg Engl. 1992; 74:59-62. [PubMed]
- Thompson A, Contreras M, Knowles S: Blood component treatment: A retrospective audit in five major hospitals. J Clin Pathol. 1991; 44:734-7. [Free full text] doi:10.1136/jcp.44.9.734
- Morrison JC, Sumrall DD, Chevalier SP, Robinson SV, Morrison FS, Wiser WL: The effect of provider education on blood utilization practices. Am J Obstet Gynecol. 1993; 169:1240-5. doi:10.1016/0002-9378(93)90289-U
- Brandis K, Richards B, Ghent A, Weinstein S: A strategy to reduce inappropriate red blood cell transfusion. Med J Aust. 1994; 160:721-2. [PubMed]
- Hasley PB, Lave JR, Kapoor WN: The necessary and the unnecessary transfusion: A critical review of reported appropriateness rates and criteria for red cell transfusions. Transfusion 1994; 34:110-5. [Free full text] doi: 10.1046/j.1537-2995.1994.34294143936
- Ghali WA, Palepu A, Paterson WG: Evaluation of red blood cell transfusion practices with the use of preset criteria. Can Med Assoc J 1994; 150:1449-54. [PubMed] [Free full text]
- World Health Organization. Blood Safety: Situation analysis. (Online) 2008 (Cited 2008 Jan 25). Available from URL:
http://www.emro.who.int/pakistan/programmeareas_bloodsafety.htm.
- World Health Organization. World blood donor day, Pakistan. (Online) 2008 (Cited 2008 Jun 16). Available from URL: http://www.who.int/worldblooddonorday/archives/2006/wbdd_pakistan/en/index.html
- Afzal S. A comparison of public and private hospital on rational use of blood in Islamabad. J Pak Med Assoc. 2013 Jan;63(1):85-9. [Free full text]
- Ismail S, Siddiqui S, Shafiq F, Ishaq M, Khan S. Blood transfusion in patients having caesarean section: a prospective multicentre observational study of practice in three Pakistan hospitals. Int J Obstet Anesth. 2014 Aug;23(3):253-9. [PubMed] [Free full text] doi: 10.1016/j.ijoa.2014.01.004
- Chawla T, Kakepoto GN, Khan MA. An audit of blood cross-match ordering practices at the Aga Khan University Hospital: first step towards a Maximum Surgical Blood Ordering Schedule. J Pak Med Assoc 2001; 51: 251-4. [Free full text]
- Bolton-Maggs PH, Cohen H. Serious Hazards of Transfusion (SHOT) haemovigilance and progress is improving transfusion safety. Br J Haematol. 2013 Nov;163(3):303-14. [PubMed] [Free full text] doi: 10.1111/bjh.12547
- Selik RM, Ward JW, Buehler JW: Demographic differences in cumulative incidence rates of transfusion-associated acquired immunodeficiency syndrome. Am J Epidemiol 1994; 140:105-12. [Free full text]
- Dodd RY: The risk of transfusion-transmitted infection. N Engl J Med 1992; 327:419-20. [PubMed] [Free full text]
- Busch OR, Hop WC, Hoynck van Papendrecht MA, Marquet RL, Jeekel J: Blood transfusion and prognosis in colorectal cancer. N Engl J Med 1993; 328:1372-6. [Free full text]
- Triulzi DJ, Vanek K, Ryan DH, Blumberg N: A clinical and immunologic study of blood transfusion and postoperative bacterial infection in spinal surgery. Transfusion 1992; 32:517-24. [Free full text] doi: 10.1046/j.1537-2995.1992.32692367194
- Mezrow CK, Bergstein I, Tartter PI: Postoperative infections following autologous and homologous blood transfusions. Transfusion 1992; 32:27-30. doi: 10.1046/j.1537-2995.1992.32192116427
- Murphy P, Heal JM, Blumberg N: Infection or suspected infection after hip replacement surgery with autologous or homologous blood transfusions. Transfusion 1991; 31:212-7. [PubMed] [Free full text]
- Edna TH, Bjerkeset T: Association between blood transfusion and infection in injured patients. J Trauma 1992; 33:659-61. [PubMed]
- Wallace EL, Surgenor DM, Hao HS, et al. Collection and transfusion of blood and blood components in the United States, 1989. Transfusion 1993;33:139-44. [PubMed] [Free full text]
- Krever H. Commission of inquiry on the blood system in Canada: final report. Ottawa, Ontario, Canada: Canadian Government Publishing; 1997.
- Practice Guidelines for blood component therapy: A report by the American Society of Anesthesiologists Task Force on Blood Component Therapy. Anesthesiology. 1996;84(3):732-47. [PubMed]
- Messmer K, Sunder-Plassmann L, Jesch F, Gornandt L, Sinagowitz E, Kessler M: Oxygen supply to the tissues during limited normovolemic hemodilution. Res Exp Med 1973; 159:152-66. [PubMed]
- Czer LSC, Shoemaker WC: Optimal hematocrit value in critically ill postoperative patients. Surg Gynecol Obstet 1978; 147:363-8. [PubMed] [Free full text]
- Delano BG, Nacht R, Friedman EA, Krasnow N: Myocardial anerobiosis in anemia in man. Circulation 1970; 42(suppl 3):148. [PubMed]
- Johansen SH, Laver MB: Cardiovascular effects of severe anemic hypoxia. Acta Anaesth Scand 1966; 24(suppl):63-8. [PubMed] doi: 10.1111/j.1399-6576.1966.tb01104.x
- Varat MA, Adolph RJ, Fowler NO: Cardiovascular effects of anemia. Am Heart J 1972; 83(3):415-26. [PubMed] doi: 10.1016/0002-8703(72)90445-0
- Viele MK, Weiskopf RB: What can we learn about the need for transfusion from patients who refuse blood?: The experience with Jehovah’s Witnesses. Transfusion 1994; 34:396-401. [PubMed] doi: 10.1046/j.1537-2995.1994.34594249050.x
- Klein AA, Arnold P, Bingham RM, Brohi K, Clark R, Collis R, et al. AAGBI guidelines: the use of blood components and their alternatives 2016. Anaesthesia. 2016 Jul;71(7):829-42. [PubMed] [Free full text] doi: 10.1111/anae.13489
- Guidelines on the Administration of Blood Components. British Committee for Standards in Haematology, 2009. [Free full text]
- Tinegate H, Birchall J, Gray A, et al. Guideline on the investigation and management of acute transfusion reactions. Prepared by the BCSH Blood Transfusion Task Force. Br J Haematol. 2012;159(2):143–53. [PubMed] [Free full text] doi: 10.1111/bjh.12017
- Hunt BJ, Allard S, Keeling D, et al. A practical guideline for the haematological management of major haemorrhage. Br J Haematol. 2015; 170: 788–803. [PubMed] [Free full text] doi: 10.1111/bjh.13580
- Blood transfusion. National Institute for Health and Care Excellence (NICE) Guideline 2015.
(accessed 23/05/2016). [Free full text]
- Major trauma: assessment and initial management. National Institute for Health and Care Excellence (NICE) guidelines [NG39]. [Free full text]
(accessed 26/04/2016).
- Klein AA, Arnold P, Bingham RM, Brohi K, Clark R, Collis R, et al. AAGBI guidelines: the use of blood components and their alternatives 2016. Anaesthesia. 2016 Jul;71(7):829-42. [PubMed] [Free full text] doi: 10.1111/anae.13489
↧
Introduction to basic transesophageal echocardiography (TEE) and standard views
Mohammad Hamid, MBBS, Diplomate American Board1, Mohammad Irfan Akhtar, MBBS, FCPS2
1Associate Professor; 2Assistant Professor
Department of Anesthesia, Aga Khan University, Karachi (Pakistan)
Correspondence: Dr Mohammad Hamid, Associate Professor, Department of Anesthesia, Aga Khan University, PW II, Stadium Road, Karachi, 74800 (Pakistan); Tel: +923486 4639; E-mail: mohammad.hamid@aku.edu
ABSTRACT
Intraoperative use of transesophageal echocardiography (TEE) for monitoring and diagnostic purposes has increased over the years in cardiac surgical patients and anaesthesiologists have taken a lead to develop expertise in performing this examination. TEE has proved to be helpful in the management of non-cardiac surgical and Intensive care unit patients particularly those patients who are haemodynamically unstable. It provides important information about ventricular and valvular anatomy and its function. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. Several guidelines have been established for performing comprehensive TEE examination and cardiologists and anaesthesiologists follow these guidelines to identify any cardiovascular abnormality.
TEE use is limited to very few centres in Pakistan, mainly due to the equipment cost and lack of expertise. In addition, there are no established TEE training institutes. The main purpose of this article is to provide basic information about transesophageal echocardiography machine, TEE probe and how to obtain standard images by probe manipulation.
Key words: Transesophageal Echocardiography; Intraoperative; Guidelines; Ultrasound;
Echocardiography, Doppler; Doppler; Ultrasonography; Diagnosis; Diagnostic Techniques and Procedures
Citation: Hamid M, Akhtar MI. Introduction to basic transesophageal echocardiography (TEE) and standard views. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S91-S96
Received: 23 May 2016; Reviewed: 30 May 2016; Corrected: 28 June 2016; Accepted: 10 July 2016
INTRODUCTION
Transesophageal echocardiography (TEE) has become an essential component of cardiac anaesthesia and its value in cardiac surgery(1) is well established. In addition, it is increasingly being used for cardiac assessment and monitoring in intensive care(2) and non-cardiac surgeries(3, 4). TEE has been used to optimize perioperative care in patients with high risk for cardiac event and for quick assessment of cardiac function and fluid status in haemodynamically unstable patients. Intraoperative use of TEE was introduced in 1980 and comprehensive guidelines for intraoperative examination were published in 1999 by American Society of Echocardiography and Society of Cardiovascular Anesthesiologists(5) (ASE/SCA). A 2-D echocardiography is the most common mode used for examination along with Doppler assessment. A 3-D examination is also evolving and gaining popularity particularly during valvular repairs(6). Guidelines for 3-D echocardiography examination have also been developed(7). ACC/AHA guidelines discourage the routine use of TEE but recommended that it can be used in emergency situations where corrective therapy for haemodynamic instability failed in non-cardiac surgery patients (Class IIa recommendation)(8).
TEE provides important information about ventricular and valvular anatomy and function. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. Main advantage of TEE is that it can be introduced even during the surgery on thoracic and abdominal region. Other advantages of TEE include the presence of transducer close to posterior structures and high resolution images due to absence of intervening lung or bones.
Echocardiography uses high frequency sound waves (also called ultrasound). As we know that sound is a form of energy that travels in waves. When a sound wave strikes a solid or fluid filled structure, some of the waves reflected back to the transducer and these reflected sound waves are called echoes. A sound wave can travel easily through gaseous structure but travel fastest through solids. Sound waves obey the law of reflection, refraction, diffraction and attenuation. Sound waves are sent through a device at the end of echo probe called transducer. A 2-D image is obtained by sweeping the ultrasound beam.
ECHO MACHINE & IMAGE OPTIMIZATION
Same machine is used for Transthoracic and Transesophageal Echocardiography. Knowledge about the echocardiography machine is an essential component of TEE examination. Several adjustments are needed to improve the quality of image and better examination. Machine has a monitor and several knobs and sliders on front panel which helps in optimization of image quality. Different knobs and their functions are explained below.
The depth should be set just beyond the structure of interest. Higher depth setting leads to reduction in size of image and also slows the frame rate because system has to wait longer for signals to be received. Once the structure of interest is visible and centred, do not increase the depth. Image gain increases the sensitivity (amplitude) of the system to the returning signals, similar to volume control in audio system. If sets too high, the image will appear bright and tissues like MV appears thickened. Too low gain will show only pericardium. It should be adjusted in such a manner that the blood appears nearly black and cardiac tissues as grey.
Time gain compensation (TGC) are several slider type panels which allow differential adjustment of gain. These should be used to eliminate artefacts and optimize the image. TGC should be used frequently. Normally TGC controls are set lower for near field and higher for the far field. Focus appears as arrow head on left side of image and should be adjusted to the level of structure of interest. If focus point is too far away from the structure of interest, the image resolution will not be adequate. Higher frequencies are used when structure is close to the transducer (Atria, AV) while lower frequencies are helpful when structure is far from transducer (Deep transgastric view).
Color gain increases or amplifies the signals generated by the returning echoes. Set color gain by increasing the color gain control until speckles of color appear outside the blood pools and then decrease the gain one to two settings until the speckles go away. Too high gain will overestimate the regurgitant jet. Sector size controls the angle of sector displayed on the monitor. This angle ranges from 15-90 degree. The most important effect of the sector size is on the frame rate. The wider the sector size, the lower the frame rate and the temporal resolution. Sector size should be kept small for fast moving objects.
Safety and precautions for TEE examination
Review the history and previous transthoracic examination before TEE examination. Insert the probe after intubation and use a bite block. Never use force when inserting the probe and always direct the probe centrally towards the back of pharynx after lifting the mandible. Use of TEE is contraindicated in patients with swallowing problems and esophageal diseases. When probe is not in use e.g. during cardiopulmonary bypass period, then either freeze the image or turn off the power. Do not insert the probe after the patient is heparinised.
TEE Probe and its Manipulation
TEE probe is basically a gastroscope with a small transducer mounted at the tip. Probe has two knobs at the handle. Larger control wheel is used for ante flexion and retro flexion while smaller wheel is used for left or rightward flexion of the tip of TEE probe. One electronic switch at the handle, scan the heart in various axial views. It ranges from 0 degree to 180 degree.
Echo probe functions on the principle of piezoelectric effect. The word originates from the Greek word “Piezein” which denotes “to press”. TEE probe contains several piezoelectric crystals (Quartz, Barium titanate, and tourmaline), which vibrate when voltage is applied. These vibrations produce sound waves which propagates in particular direction. These waves can be directed as a beam and returning signals again change the shape of crystals which emit electrical signals. These echoes are converted into the cardiac images on the monitor.
Movement of TEE probe
Quality of image can be improved by using a larger control wheel on the handle which provides angulation (Ante flexion or retro flexion) while smaller knob is used for tilting the probe laterally (Left or right). Whole probe can also be turned clockwise and ante clockwise (called turning right or left). Rotation of whole Image plane is possible by controlling the axis rotation between the range of 0 -180 degrees. It is called rotating forward if the angle moved from 0 degrees towards 180 degrees.
STANDARD VIEWS (Figure 1)
ECHO is a two dimensional (cross section) representative of anatomical structure which exists in three dimensions in space. A 2D image obtained in a transverse plane at 0° is perpendicular to the shaft of transducer while at 90° it lies in the vertical plane and runs parallel to the shaft of probe.
Short axis means the image is perpendicular to anatomical structure and long axis is parallel to structure of interest. Apex of the image is close to the probe while arc of the image sector shows more distal structures. Each structure must be examined in multiple planes if possible.
ASE/SCA task force has developed guidelines of intraoperative echo examination and recommends 20 standard images. These guidelines were revised in 2014 and 8 more standard views are added(9). Reeves et al. have suggested only 11 views for basic TEE examination during perioperative period and in the intensive care unit patients(10).
Consent is taken from all the patients before examination and for the procedural sedation propofol is commonly used(11). Study begins by inserting ECHO probe to mid esophagus (ME) which is about 35cm from incisors. It is suggested to push TEE probe into stomach after mid esophageal examination and finally pulled out in upper esophagus.
MIDESOPHAGEAL (ME) VIEWS
In the mid esophagus position, the transducer is just behind the left atrium. Keep the angle at 0° degree and move the probe up and down to obtain Four chamber view. Structures seen are left atrium (LA), left atrial appendage (LAA), right atrium (RA), RV, LV (Septal & Lateral wall), mitral valve (MV) and tricuspid valve (TV). After obtaining four chamber view rotate the axis from 0° to 60-70 degree and you will be able to see LA, LV and MV. This view (Mitral Commissure view) is mainly used for assessment of MV pathology. Further 90° rotation (Range 80-100) will provide Two chamber view and shows the LA, LAA, MV and anterior & inferior walls of LV. At this position if we turn the probe towards left side pulmonary veins (left sided) becomes visible. Use color flow to confirm this finding.
From four chamber view create an angle of 135° (Long axis (LAX) view, Range 120-160°) and you will be able to visualize LA, LV, LVOT, Aortic valve, MV and ascending aorta. Two cusps of aortic valve will be visible in this view. From four chamber view withdraw the probe slightly and rotate 40° (AV short axis view, range 30 – 60) to see Mercedes Benz sign (Figure 1) of aortic valve. Right coronary cusp (RCC) is facing towards RV and LCC at right of screen. Non coronary cusp, Interatrial septum and RV outflow tract are also visible.
Image 1: AV short axis view showing Aortic valve in closed position with three aortic cusps in the middle
From AV short axis view rotate further 80 degrees (RV inflow – outflow view) to see RA, TV, RV, RV outflow tract, pulmonary Valve and main Pulmonary artery. This view is very helpful in tetralogy of Fallot repair. Turn the probe right and rotate at about 110° (Bicaval view, Range 80 – 110° from AV SAX) and watch SVC, IVC, RA, LA, interatrial septum, Eustachian valve (Figure 2). This view is used to confirm the position of the tip of central venous pressure (CVP) line. Right pulmonary vein can also be visualized in this view by turning the probe to right side.
Image 2. Bicaval view showing SVC on right side and IVC on left side
AV long axis view is obtained by rotating from AV SAX view to 120 -160°. You will be able to see Proximal ascending aorta, LV outflow, MV, AV, Lower most RCC and adjacent to anterior MV leaflet is non coronary cusp. Withdraw TEE probe slightly from AV SAX view and rotate about 40° (Ascending aorta short axis view) to see proximal ascending aorta, Main pulmonary artery, right pulmonary artery and SVC.
Further rotation to around 130° will give you Long axis view of Ascending called Ascending aorta long axis view. Aorta along with Right pulmonary artery (short axis) will be visualized.
Transgastric view (TG)
From the mid esophagus position pushed down the probe, so that the tip of the TEE probe is in the stomach (40-45 cm from incisor). Now anteflex the tip of TEE probe to assess ventricle from base to apex.
In this view (TG basal short axis view (0°)) the basal portion of the ventricle and MV should be visible. This view is helpful in detection of basal LV ischaemia and assessment MV pathology. TG Mid SAX view (0° range 0-15) is obtained by advancing the probe slightly and then anteflexion at the tip. Posteromedial papillary muscle can be appreciated at 1° O’clock and anterolateral muscle at 5° O’clock position. This view is useful for monitoring global LV function. Ejection fraction estimation can be done with the help of M-Mode in this view. This view is most important in detecting myocardial ischemia in different coronary artery territory.
From the mid TG view rotation of axis to 90° will show the Anterior (bottom) and inferior walls of left ventricle. This view is called TG two chamber view. By turning the whole probe clockwise will show you the right atrium and tricuspid valve. This image is called TG right ventricular inflow view.
Now advance the probe deep into the stomach then sharply anteflex and at the same time withdraw slowly to see Deep TG long axis view (0° about 45 -50 cm from incisor). This will show all four chambers, AV and LVOT. This view is basically used for doppler (CWD) examination to estimate velocities across AV. Finally, TG long axis view is visualized by rotating 120° from mid SAX view. Left ventricle in long axis and LVOT are clearly seen in this view.
Upper esophageal (UE) view (20-25 cm from incisor)
For visualization of great vessels reduce the screen depth to 6 cm and withdraw TEE probe gradually to ME four chamber view. Now turn the probe anticlockwise to find descending thoracic aorta SAX view at 0° and descending thoracic aorta LAX view at 90°.
Withdraw the probe further until distal aortic arch is seen then follow the arch by turning the probe towards right side. This is upper esophageal aortic arch LAX view at 0°. When transducer rotates to 90° UE aortic arch SAX view is seen. Origin of left subclavian artery is also seen.
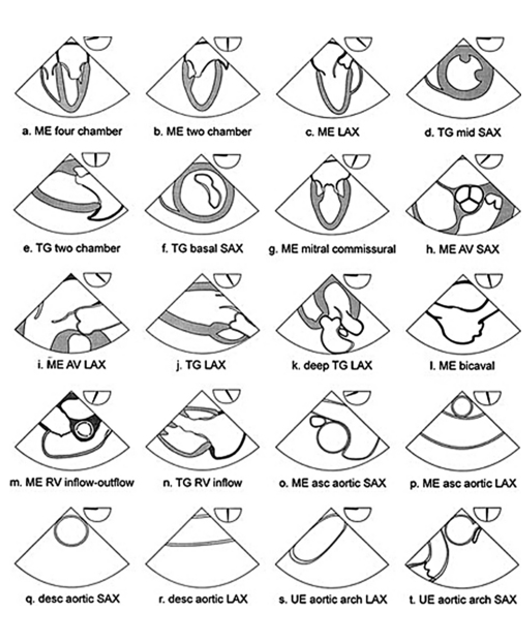
Figure 1: American society of echocardiography and Society of cardiovascular anesthesiologist recommended 20 cross sectional views for comprehensive TEE examination. ME= mid esophagus, LAX= long axis, SAX= short axis, TG= transgastric, AV= aortic valve, RV= right ventricle, asc = ascending, des= descending, UE= upper esophageal.
Left ventricle wall motion abnormalities: (Figure 3)
Left ventricle wall motion abnormalities can be detected by using 16 segments model as suggested by SCA/ASE. It consists of six basal segments, six segments at mid papillary level and four segments at apical level. Four chambers view, Two chambers view, TG basal SAX view, TG mid SAX view can provide information about all 16 segments. Involved coronary artery (Stenosed or Blocked) can be identified by looking at the regional wall motion abnormalities in these segments. The qualitative grading of wall motion is Normal (>30% thickening), Mild hypokinetic (10 – 30% thickening), severely hypokinetic (<10% thickening), Akinetic (No thickening) and dyskinetic (Moves paradoxically).
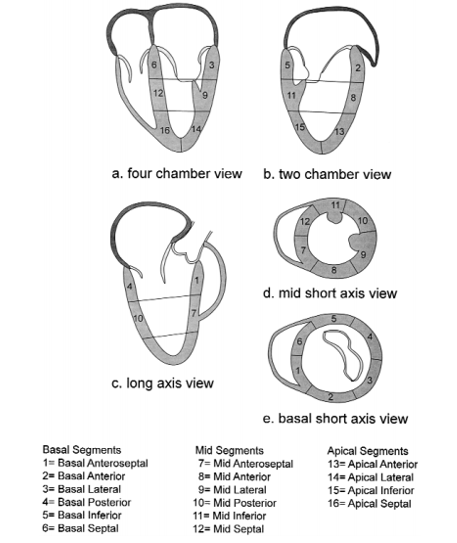
Figure 2: Sixteen segment model of the left ventricle.
DOPPLER EXAMINATION
It is a method of detecting the direction and velocity of moving blood within the heart and vessels. Doppler principle is used to understand the movement of blood and tissues in the body. Pressure gradients are derived by using Doppler analysis of blood flow. Doppler examination includes:
Pulsed wave Doppler (PWD)
Same transducer crystal is used for transmission and reception. It allows sampling of blood flow velocities from a specific intracardiac depth. PWD can measure only limited range of velocities. Flow velocity through the mitral valve can be easily detected by PWD.
Continuous wave Doppler (CWD)
Two crystals transducers are used, one continuously transmits and other continuously receives and processed the signals. Very high velocities like aortic stenosis can be measured. Blood flow along the entire beam is observed.
Color flow Doppler (CFD)
Different colors are used to designate the direction of blood flow. Red color is seen when blood flowing towards the probe while the blue color denotes the flow away from the probe. Mosaic pattern represent turbulent flow, usually seen when there is valvular stenosis or regurgitation.
INTRAOPERATIVE APPLICATION OF TEE IN ADULT CARDIAC SURGERY
TEE application in the intraoperative period is very important in the assessment of the biventricular function, cardiac fluid status, valvular repair accuracy, para-valvular leak, residual septal defect and intra-cardiac air. It plays an important complementary role with PAC in the successful management of high-risk cardiac surgical patients.
BASIC PERIOPERATIVE TEE EXAMINATION FOR NON CARDIAC SURGERY
Out of 20 cross sectional views used for comprehensive examination, seven can be utilized for basic TEE examination for non-cardiac surgery. These includes ME 4 chamber, ME two chamber, ME long axis, Transgastric mid SAX, ME RV inflow-outflow, Descending aortic SAX and upper esophageal aortic arch LAX view. This approach of perioperative TEE is proposed to improve time efficiency and diagnostic yield.
CONCLUSION
Improved outcomes have been seen after the introduction of Transesophageal echocardiography in cardiac surgery, particularly in the valve surgery. It provides valuable information about the anatomy and function of different chambers of heart and valves. Blood flow and velocity across the valves and in large vessels can also be identified. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. It is important to know the various knobs on TEE machine and probe for better visualization of heart structures. Guidelines for comprehensive intraoperative TEE examination are also available for anaesthesiologists. These guidelines provide information about the TEE machine, probe insertion technique and how to manipulate probe to identify a particular structure. Doppler is also one of the important component of TEE examination which helps to detect the direction and velocity of moving blood within the heart and vessel.
Acknowledgement: We acknowledge the permission from Anesth Analg (Reference #5) for allowing us to use Figure 1 and 2 in this article
Conflict of interest: No conflict of interest declared by the authors
Authors’ contribution: KS & MH: Concept, Design, Literature search, Manuscript preparation & review
REFERENCES
- Klein AA, Snell A, Nashef SA, et al. The impact of intra-operative transoesophageal echocardiography on cardiac surgical practice. Anaesthesia 2009;64:947-952 [PubMed] [Free full text] doi: 10.1111/j.1365-2044.2009.05991.x.
- Maxwell C, Konoske R, Mark J. Emerging Concepts in Transesophageal Echocardiography. F1000Res. 2016:1-10. [PubMed] [Free full text] doi: 10.12688/f1000research.7169.1.
- Rebel A, Klimkina O, Hassan ZU. Transesophageal echocardiography for the noncardiac surgical patient. Int Surg 2012;97:43-55 [PubMed] [Free full text] doi: 10.9738/CC61.1.
- Guarracino F, Baldassarri R. Transesophageal echocardiography in the OR and ICU. Minerva Anestesiol 2009;75:518-529 [PubMed] [Free full text]
- Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. Anesth Analg 1999;89:870-884 [PubMed]
- Mahmood F, Jeganathan J, Saraf R, Shahul S, Swaminathan M, Mackensen GB, et al. A Practical Approach to an Intraoperative Three-Dimensional Transesophageal Echocardiography Examination.J Cardiothorac Vasc Anesth 2016;30:470-490 [PubMed] doi: 10.1053/j.jvca.2015.10.014.
- Lang RM, Badano LP, Tsang W, Adams DH, Agricola E, Buck T, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. J Am Soc Echocardiogr 2012;25(1):3-46 [PubMed] doi: 10.1016/j.echo.2011.11.010.
- Shillcutt SK, Markin NW, Montzingo CR, Brakke TR. Use of rapid “rescue” perioperative echocardiography to improve outcomes after hemodynamic instability in noncardiac surgical patients. J Cardiothorac Vasc Anesth 2012;26:362-370 [PubMed]
doi: 10.1053/j.jvca.2011.09.029.
- Hahn RT, Abraham T, Adams MS, Bruce CJ,Glas KE, Lang RM, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2013;26(9):921-64 [PubMed] doi: 10.1016/j.echo.2013.07.009
- Reeves ST, Finley AC, Skubas NJ, et al. Basic perioperative transesophageal echocardiography examination: a consensus statement of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2013;26(5):443-456 [PubMed] doi: 10.1016/j.echo.2013.07.009.
- Akaishi M, Asanuma T, Izumi C, Iwanaga S, Kawai H, Daimon M, et al. Guidelines for conducting transesophageal echocardiography (TEE): Task force for guidelines for conducting TEE: J Echocardiogr. 2016;14(2):47-8 [PubMed] doi: 10.1007/s12574-016-0281-9
↧
Perioperative cardiac arrest: teamwork and management
Abhijit Nair1, Vibhavari Naik1, Basanth Kumar Rayani2
1Consultant Anesthesiologist; 2Chief Anaesthesiologist
Department of Anesthesiology, Basavatarakam Indo-American Cancer Hospital and Research Institute, Hyderabad, Telangana 500034, (India)
Correspondence: Dr Abhijit Nair, Department of Anesthesiology, Basavatarakam Indo-American Cancer Hospital and Research Institute, Road No 10, Banjara Hills, Hyderabad, Telangana 500034, (India); Phone: 040-23551235; E-mail: abhijitnair95@gmail.com
ABSTRACT
Perioperative cardiac arrest is an unfortunate event that can have disastrous outcomes if not attended and intervened on time. Arrests occurring intraoperatively have usually good outcomes as the patient is continuously monitored and it is easy to find out the cause of cardiac arrest. Patients coming for emergency surgeries, advanced ASA physical status, extremes of age groups (geriatric, pediatric) are the candidates in which perioperative cardiac arrest occurs. Events precipitating cardiac arrests should be identified early in wards. However once an arrest occurs in wards, the overall outcome depends on the timing, efforts of the resuscitation team and the events leading to cardiac arrest.
Key words: Perioperative; Cardiac arrest; Anesthesia; Mortality; Intraoperative
Citation: Nair A, Naik V, Rayani BK. Perioperative cardiac arrest: teamwork and management. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S97-S105
Received: 20 August 2016; Reviewed: 12 September 2016; Accepted: 23 September 2016
INTRODUCTION
Managing unexpected perioperative events can be challenging for the attending
anesthesiologist. Although few events might be anticipated in sick patients, a thorough preoperative evaluation for an elective surgery doesn’t always guarantee that nothing will go wrong. Unexpected events can compromise patient safety or turn out to be life threatening if appropriate equipment, protocols and help are not readily available.
To analyze this, a symposium issue was published by Anesthesia and Intensive Care in 1993 after the Australian Incident Monitoring Study (AIMS) that was started in 1988. The paper reviewed 2000 incidents presented in 30 papers that addressed different types of anesthetic incidents like anaphylaxis, difficult intubation, cardiac arrest, wrong drug administration.1
There is no uniform definition for perioperative cardiac arrest (POCA) in literature. As the terminology implies, POCA is a cardiac arrest occurring during induction of anesthesia, intra-operatively or post-operatively.2 Any POCA happening after 24 hours of surgery can be of anesthetic or non-anesthetic etiology. Cardiac arrest due to accidental or wrong drug administration or inadvertent intravenous local anesthetic injection can also be considered under anesthetic etiology. Any event which requires chest compressions perioperatively should be considered as a POCA.
Cardiac arrest occurring in the perioperative period is a potentially reversible event. In hospital cardiac arrest has better outcomes compared to the cardiac arrests occurring in the community that are not witnessed. This is due to the availability of monitoring, equipment for resuscitation and trained personnel in the hospital. The incidence of POCA is varied in different parts of the world, ranging from 3-163 per 10,000 surgeries. This difference could be due to different patient types, available facilities, infrastructure and efficiency of support system, which gets reflected in the morbidity/mortality/ adverse event statistics. Although the incidence of anesthesia related cardiac arrest is reducing all over the world due to modern equipment, mandatory training in resuscitation and simulator based learning, the overall incidence of POCA remains more or less the same. This could be due to patients with advanced ASA physical status, emergency surgeries and more complex procedures due to advances in the field of medicine. In a prospective study done by Sebbaq et al3 involving 40,379 anesthetics between January to December 2007, 52 patients had cardiac arrest intraoperatively. Though 69% patients had return of spontaneous circulation after the initial arrest, 30 day survival was seen in only 25% of patients.
The factors responsible for such a short survival rate were found to be: ASA physical status IV and V, emergency surgery, hemorrhagic events, hypovolemia and use of atropine during resuscitation. Dedicated team work can have favorable results when it is applied to perioperative care of surgical patients, especially the sick ones (emergency surgeries, elderly patients, patients with advanced ASA physical status, neonates and infants). The team should involve the operating surgeon, anesthesiologists and the specialists who were involved in patient’s care perioperatively (e.g. cardiologist, nephrologist, pulmonologist, obstetrician, oncologist etc.). The team should meet to discuss the patient’s progress and to decide the management plan till the patient gets discharged from the hospital. Anesthesiologist forms an important link for coordinating the team.
LITERTURE REVIEW
In the studies involving interpretation of prospective or retrospective data related to perioperative cardiac arrest, the incidence was particularly higher in emergency surgeries compared to elective surgeries.4 This is seen because the emergency surgical patient comes to operation theatre without detailed preoperative workup and thus is not optimized compared to the elective counterpart . The other area which was striking after reviewing literature was the extremes of age (geriatric patients and neonates).5,6 Even though elective surgical patients are thoroughly worked up, factors like prolonged surgery, advanced ASA physical status, perioperative blood transfusions, acute kidney injury, electrolyte imbalances, ventilatory support, nosocomial infections etc. are not always predictable. All the above mentioned factors either alone or in combination could be held responsible for triggering or predisposing to cardiac arrest.
All the data of perioperative and intraoperative deaths published in indexed journals have been collated. To collect this information we searched Pubmed, Medline, Scopus, Embase with following keywords: perioperative, cardiac arrest, anesthesia, mortality and intraoperative.
In all we have presented a summary of 12 papers published in reputed journals in a tabular form (Table 1). We have mentioned the type of study (retrospective, prospective, observational), the type of event described in the paper i.e. perioperative, intraoperative or both, the time frame in which the analysed data was collected and the incidence of mortality derived in that particular paper.
Table 1: A summary of 12 papers published7-18
| No. | Authors | Type of study | Type of event | Duration of data | Incidence |
| 1. | Siriphuwanun et al | Retrospective cohort | Within 24 hrs of anaesthesia | 8 yrs (from 2003-2011): 44,339 patients | 163/10,000 |
| 2. | Tamdee et al | Retrospective | Perioperative | Between 2003-2007. | Incidence of 24-hour perioperative cardiac arrest : 40.4/10,000 |
| 3. | Siracuse et al | Retrospective (National Surgical Quality Improvement Program data ) | Perioperative
( Vascular surgery ) |
3 yrs
( 2007-2010 ) |
1% patients
( out of 123,581 patients, 1234 patients had cardiac arrest ) |
| 4. | Nunes et al | Retrospective data ( from teaching hospital ) | Perioperative | 15 yrs
( 1996-2010) |
54.44/10,000 anesthetics |
| 5. | Kazaure et al | Retrospective cohort study(American College of Surgeons–National Surgical Quality Improvement Program) | Perioperative | 6 yrs
(2005-2010) |
1 in 203 surgical cases |
| 6. | Braz et al | Retrospective data | Perioperative | 9 yrs
(1996-2005) |
34.6/10,000 |
| 7. | Goswami et al | Prospective
(American College of Surgeons National Surgical Quality Improvement Program database) |
Intraoperative | 3 yrs
(2005-2007) |
7.22/10,000 |
| 8. | Messahel et al | Retrospective | Perioperative | 18 yrs
(1992-2010) |
0.03%
( 3/10,000)
|
| 9. | Vane et al | Retrospective ( a review of data from tertiary and academic hospitals) | Intraoperative | Included studies conducted between 1982-2007. | Incidence changed from 39/10,000 to 13/10,000 in the duration of 25 yrs |
| 10. | Nunnally et al
|
Retrospective
(National Anaesthesia Clinical Outcomes Registry)
|
Perioperative
|
4 yrs ( 2010-2013)
|
5.6/10,000
|
| 11. | Gonsalez et al | Observational | Intraoperative and perioperative (pediatric patients ) | 2005-2010 | Incidence of cardiac arrest 20.65/10,000, incidence of death 10.32/10,000 |
| 12. | Bharti et al | Retrospective | Perioperative | 2003-2008 | Anaesthesia
related mortality :1.2/10 000 , 7.7/10 000 anaesthetics with a survival rate of 56%. |
Runciman et al19 reviewed 4000 incidents reported to Australian Incident Monitoring Study and identified 24 specific anaesthesia crisis situations. With the help of teams of practising anaesthesiologists, they developed management algorithms. The authors had first published the algorithm in 1993 and in 2005 they reemphasized the importance of using these algorithms. The algorithms provide a clear insight on how to approach a crisis during anaesthesia management. Having such algorithms in operation room (OR) /ICU as a ready reference can be useful (Table 2). The algorithm is named as “COVER ABCD – A SWIFT CHECK”. COVER includes circulation, oxygen, ventilation / vaporises, endotracheal tube and review. ABCD is airway, breathing, circulation, drugs as in ACLS. “A SWIFT CHECK” pneumonic is for differential diagnosis to short list the cause of event, similar to 5H’s and 5T’s in ACLS course.
Table 2: Crisis management algorithm: ‘COVER ABCD’
| C1 | Circulation | Establish adequacy of peripheral circulation (rate, rhythm and character of pulse). If pulseless, institute cardiopulmonary resuscitation (CPR). The core algorithm must still be completed as soon as possible. |
| C2 | Colour | Note saturation. Examine for evidence of central cyanosis. Pulse oximetry is superior to clinical detection and is recommended. Test probe on own finger, if necessary, whilst proceeding with O1 and O2. |
| O1 | Oxygen | Check rotameter settings, ensure inspired mixture is not hypoxic. |
| O2 | Oxygen analyser | Adjust inspired oxygen concentration to 100% and note that only the oxygen flowmeter is operating. Check that the oxygen analyser shows a rising oxygen concentration distal to the common gas outlet. |
| V1 | Ventilation | Ventilate the lungs by hand to assess breathing circuit integrity, airway patency, chest compliance and air entry by ‘‘feel’’ and careful observation and auscultation. Also inspect capnography trace.
|
| V2 | Vaporiser | Note settings and levels of agents. Check all vaporiser filler ports, seatings and connections for liquid or gas leaks during pressurisation of the system. Consider the possibility of the wrong agent being in the vaporiser. |
| E1 | Endotracheal tube | Systematically check the endotracheal tube (if in use). Ensure that it is patent with no leaks or kinks or obstructions. Check capnograph for tracheal placement and oximeter for possible endobronchial position. If necessary, adjust, deflate cuff, pass a catheter, or remove and replace. |
| E2 | Elimination | Eliminate the anaesthetic machine and ventilate with self-inflating (e.g. Air Viva) bag with 100% oxygen (from alternative source if necessary). Retain gas monitor sampling port (but be aware of possible problems). |
| R1 | Review monitors | Review all monitors in use (preferably oxygen analyser, capnograph, oximeter, blood pressure, electrocardiograph (ECG), temperature and neuromuscular junction monitor). For proper use, the algorithm requires all monitors to have been correctly sited, checked and calibrated. |
| R2 | Review equipment | Review all other equipment in contact with or relevant to the patient (e.g. diathermy, humidifiers, heating blankets, endoscopes, probes, prostheses, retractors and other appliances). |
| A | Airway | Check patency of the non-intubated airway. Consider laryngospasm or presence of foreign body, blood, gastric contents, nasopharyngeal or bronchial secretions. |
| B | Breathing | Assess pattern, adequacy and distribution of ventilation. Consider, examine and auscultate for bronchospasm, pulmonary oedema, lobar collapse and pneumo- or hemothorax. |
| C | Circulation | Repeat evaluation of peripheral perfusion, pulse, blood pressure, ECG and filling pressures (where possible) and any possible obstruction to venous return, raised intrathoracic pressure (e.g. inadvertent PEEP) or direct interference to (e.g. stimulation by central line) or tamponade of the heart. Note any trends on records.
|
| D | Drugs | Review intended (and consider possible unintended) drug or substance administration.
Consider whether the problem may be due to unexpected effect, a failure of administration or wrong dose, route or manner of administration of an intended or ‘‘wrong drug’’. Review all possible routes of drug administration. |
(Table reproduced with permission from the publisher, BMJ Publishing Group Ltd.; license number: 3874521013406)
Table 3: ‘A SWIFT CHECK’ checklist
| Condition | Comments | |
| A | Air embolus | Hypotension, hypocarbia |
| A | Anaphylaxis | Hypotension, bronchospasm, urticaria |
| A | Air in pleura | Pneumothorax, circulatory/ respiratory deterioration |
| A | Awareness | Dilution of anesthetic agents |
| S | Surgeon/situation | Vagal stimulus, cord compression, bleeding, myocardial stimulation |
| S | Sepsis | Hypotension, desaturation, acidosis, hyperdynamic circulation |
| W | Wound | Trauma, bleeding, tamponade, pneumothorax, retractors |
| W | Water intoxication | Electrolyte imbalance, fluid overload |
| I | Infarct | Myocardial conduction/ rhythm problem, hypotension, poor cardiac output |
| I | Insufflation | Vagal tone, gas embolism, reduced venous return |
| F | Fat syndrome | Desaturation, hypotension |
| F | Full bladder | Sympathetic stimulation |
| T | Trauma | Spinal injury, diaphragmatic injury, ruptured viscus |
| T | Tourniquet down | LAST, bleeding |
| C | Catheter/IV cannula/chest drain | Leaks, obstruction, wrong connection, wrong rate |
| C | Cement | Hemodynamic changes with methyl acrylate |
| H | Hyper/hypothermia | Tachy/bradycardia, ECG changes |
| H | Hypoglycemia | Fasting, beta blockers, preop inadvertent insulin |
| E | Embolus | Fat, amniotic fluidà hypotension, hypocarbia, ECG changes |
| E | Endocrine | Thyroid, adrenal, pituitary, pancreas |
| C | Check | Right patient, right operation, right surgeon |
| C | Check | Case notes, preop status, drugs, diseases
|
| K | K+ | Potassium and other electrolyte : ECG changes, CNS signs |
| K | Keep | Keep the patient asleep until a new anesthetic machine can be obtained |
INTRA-OPERATIVE CARDIAC ARRESTS:20
Intraoperative cardiac arrests i.e. the cardiac arrests occurring during induction of anaesthesia, intraoperatively and immediate post-operatively (after extubation or after shifting to ICU) are always noticed events because the patient is continuously monitored and have good outcomes if addressed on time. Following are the most frequent causes of intraoperative cardiac arrest (Table 3).
- ASA Physical Status
Patients with advanced ASA have several systemic co-morbidities which can decompensate during induction of anaesthesia or perioperatively. Elderly patients and pediatric patients with underlying medical problems are the group of patients that are susceptible for POCA.
- Emergency Surgery:
The incidence of POCA is more than twice for a patient who has an emergency surgical intervention. These are the patients who are unoptimized. A thorough medical workup and assessment is not possible especially if the surgery is lifesaving. In such situations, hemodynamic events and respiratory issues encountered are more. Emergency surgical intervention is usually carried out in odd hours when the medical and surgical staff are less and an urgent help is not available in case of a life threatening event.
- Ventilation Related:
Having a CVCI (cannot ventilate, cannot intubate) situation is a nightmare for the anaesthesiologist. However if one encounters a CVCI, an alternative plan for ventilation and oxygenation should be available in the OR premises (supraglottic airways, jet ventilator, cricothyrotomy kit). A team work involving a second anesthesiologist, technician and surgeon – knowing their role in the airway plan is important. If hypoxia is unaddressed by alternative means, cardiac arrest is inevitable especially in neonates/ infants and sick patients.
- Local Anaesthesia Systemic Toxicity (LAST):
LAST is potentially life threatening event which can have disastrous outcomes. With the use of ultrasound for peripheral nerve blocks, regional anaesthesia has become safe but in spite of that case reports and series are published from centres were ultrasound is used in high volumes and has been used for years . Applying principles of ACLS and having lipid infusion in hand can prevent mortality. Bretylium is not available everywhere and a provision for emergency cardiopulmonary bypass is not possible in all hospitals (especially in non- cardiac centres). A high degree of clinical suspicion and applying principles of ACLS is important when one encounters LAST. Team work is important in such situations.
- Excessive Parasympathetic Tone:
Bradycardia/ asystole happening due to excessive parasympathetic tone is usually transient if addressed and rectified. In neonates/infants/pediatric patients, it can be treated with a dose of anticholinergic drug (atropine, glycopyrrolate). In adults, the bradycardic response is seen during port insertion for laparoscopic surgeries, peritoneal stretching during abdominal surgeries and at times as a laryngoscopic response.
- Medication-related:
Induction agents like propofol when given in usual doses to sick patients can lead to worsening of LV function, excessive vasodilatation, refractory hypotension eventually leading to cardiac arrests. This can be avoided by selecting the induction agent carefully for every patient. Etomidate, inhalational induction or induction using a benzodiazepine with narcotic combination can be useful in such situations. In sick and hypovolemic patients, even spinal/ epidural anaesthesia can lead to major adverse cardiac event due to vasodilatation leading to shock. If such situations are not addressed on time, the end result is a cardiac arrest. Excessive doses of narcotic, extubation in a deep anaesthetic plane can also lead to airway obstruction leading to cardiac arrest if not monitored and planned properly. The consequences of wrong drug administration can be catastrophic and life threatening.
- Sepsis/ SIRS:
Presence of septic focus and having SIRS or impending sepsis are usually patients coming for emergency or urgent surgeries. During surgery when handling the focus of infection, bacterial endotoxinemia and release of inflammatory mediators (IL-6, cytokines) can present with serious hemodynamic events which can precipitate cardiac arrest intraoperatively or post operatively. Careful induction, having invasive lines and proper empirical antibiotic administration if cultures are not available should be the strategy in such patients.
- Miscellaneous:
Prolonged surgery (more than 4-6 hours), massive blood transfusion, surgery in odd hours like emergency surgeries where urgent help is not available and prolonged intraoperative hypotension are other important factors that are responsible for POCA. These factors should be considered as possibilities either alone or in combination when one is investigating a POCA.
Table 4: Most frequent causes of POCA and the common location of its occurrence
| Etiology | Location |
| ASA physical status | OR/ ICU/wards |
| Emergency surgery | OR/ICU |
| Ventilation (CVCI / postextubation laryngospasm) | OR/ICU |
| LAST (local anaesthesia systemic toxicity) | OR/ICU/ wards |
| Excessive sympathetic tone | OR |
| Medication errors | OR/ICU/ wards |
| Sepsis / SIRS | OR/ICU/ wards |
| Miscellaneous (duration, intra-operative hypotension, blood transfusion) | OR/ICU/ wards |
Following are the general resuscitation principles which should be strictly adhered to, whenever a cardiac arrest occurs in the operation theatre premises.19
- Apply the algorithm of COVER ABCD – A SWIFT CHECK
- Inform the surgeon and stop the ongoing surgery
- If prone or lateral decubitus, turn the patient supine
- Apply principles of Basic/ advanced life support if cardiac arrest is confirmed
- Analyse the rhythm
- Consider intubation and ventilation with 100% oxygen if not already intubated
- Discuss differential diagnosis and plan manage accordingly
CARDIAC ARRESTS IN WARD
After getting shifted, on the ward the patients are monitored on an hourly or an intermittent basis. Very rarely, continuous monitoring occurs. If the early warning signs are ignored, the results can be catastrophic. Surgical problems like bleeding can be addressed by exploration, if the patient is resuscitated well and shifted to the OR on time. However, medical problems can have equivocal outcomes. Complications like pulmonary embolism, major adverse cardiac events, arrhythmias, stroke can have poor outcomes unless addressed early. Although considerable improvement has been in the last decade, neurological deficits were common in patients who survived resuscitation after cardiac arrest occurring on the ward.21 The reason for ROSC could be improvement in standards of resuscitation because of compulsory training of all personnel involved in acute care (physicians, anesthesiologists, intensivists, surgeons, nursing staff working in critical areas or high dependency areas and paramedics).
If the rhythm on the monitor is a shockable (VT/VF), early defibrillation can lead to a successful ROSC (return of spontaneous circulation). However if ROSC occurs after more than 30 min of resuscitation, the outcome is usually poor due to hypoxic brain damage.
CODE BLUE TEAM
Code blue is a communication system used to indicate and alert the healthcare professionals, about a patient at a particular location in the hospital who needs resuscitation. The code is activated by an internal telephone system, pagers and loudspeaker announcement in the hospital.22 A properly established code blue system reflects the organisational efficacy of the hospital. An audit of the code blue events can provide information about the areas of resuscitation which needs improvement. Frequent simulation based training and mock drills can help in practising the skills and algorithms of resuscitation.23
The reason for activating a code could be a respiratory arrest, cardiac arrest or a peri-arrest situation. The team members are expected to reach the location with all resuscitation equipment including a defibrillator and apply the principles of advanced cardiopulmonary life support. The team usually involves an anaesthesiologist, emergency physician, surgeon, cardiologist, trained nursing staff, respiratory therapist or a technician (ICU, anaesthesia). On arrival the team should be able to perform high quality chest compressions, ventilation either with bag/mask or definitive airway, drug administration, defibrillation etc. Rhythm analysis is a very important part of CPR after good quality chest compression. Identifying a shockable rhythm and defibrillating with the correct energy (in Joules) can lead to a successful resuscitation. Post resuscitation care in an appropriate critical care area is equally important.
TEAMWORK IN A PERIOPERATIVE PATIENT
Team dynamics:
A team is a group of individuals working towards a common goal. A well-orchestrated team effort would not have a better application than in a perioperative cardiac arrest, which is a potentially reversible one. ACLS course describes the importance of the role of team dynamics in carrying out a successful resuscitation. Similarly, in an OR complex any cardiac arrest should be managed by following effective resuscitation team dynamics. As OR is a restricted area, all code blue team members might not be able to enter the complex. A code blue is not always activated when an event occurs in the OR as an anaesthesiologist is always available and the patient is being monitored.
The following are the elements of effective resuscitation team dynamics described in the ACLS course24
- Closed- loop communications
- Clear messages
- Clear role and responsibilities
- Knowing one’s limitations
- Knowledge sharing
- Constructive intervention
- Re-evaluation and summarizing
- Mutual respect
The team dynamics can be continuously improved by conducting simulation training or mock drills in the operating room setting. Simulators help to imitate or rehearse perioperative life threatening events. Appropriate communication with other members of the team, decision making and implementation can be practised and replicated in an interactive manner. Simulation can be interrupted for teaching or discussion so that the skills are reinforced.25,26
The non-medical team members should also be trained in basic life support so that they can also be the part of resuscitation during a critical incident. During mock drills and simulator sessions, the role of a team member should be specifically assigned so that every member knows what is expected of them in real time during an incident.27
Lerner et al28 had proposed that a healthcare system that supports effective teamwork can improve the quality of patient care and reduce workload issues that cause burnout among healthcare professionals. However, this teamwork concept can be successful only if all team members follow the code of conduct of team dynamics. Regular audit should be performed for evaluating the practices and suggesting improvement.
Anaesthesiologist as a perioperative physician:29,30
Anaesthesiology is a multifaceted discipline. An anaesthesiologist should have knowledge of basic medical sciences, pathophysiology relevant to all diseases, implications of surgical intervention on homeostasis along with the syllabus of anaesthesiology. During pre-anaesthesia check-up, the anaesthesiologist does a thorough general, physical and systemic examination. The patient is advised further evaluation by specialists when indicated. Intraoperatively the anaesthesiologist monitors and maintains the normal physiology of the patient and addresses the critical care issues in postoperative period Anaesthesiologist is also involved in preventing perioperative surgical site infections, managing respiratory and perioperative nutrition related issues. In a recently published review by Wacker et al, the authors have summarised the preventable causes of perioperative adverse events. They have mentioned that an anaesthesiologist is a dynamic perioperative physician and are considered as pioneers in patient safety. They should be take lead in perioperative care of patients especially the sick ones so that potentially avoidable events can be prevented.
Follow-up on the wards:
A sick patient requiring emergency surgery, a patient with multiple co-morbidities, a patient who had a stormy post-operative course (massive blood loss, MACE, airway emergency, anaphylaxis etc) are the patients who might have a cardiac arrest post-operatively. Due to this reason, the team of doctors involved in the care (anaesthesiologists, surgeons, intensivist, pulmonologist, nephrologist and cardiologist) usually have to follow up at least once daily depending upon the type of co-morbidity. The nursing staff should be trained to use MEWS (Modified Early Warning System) to identify a predisposing factor which could lead to a cardio-respiratory event. A score of 5 or more than 5 has been shown to be responsible for higher possibility of a life threatening event leading to ICU admission.31
If a postoperative patient ends up in a cardiac arrest on the ward, it is usually the anaesthesiologist who is the team leader conducting the resuscitation and managing the patient if further surgical intervention is required. It would be ideal if the anaesthesiologist could visit the sick patients who are transferred from the ICU to the ward at least once a day. During such visits, early signs of deterioration may be picked up and addressed appropriately.\
CONCLUSION
In spite of advances in healthcare, compulsory training for doctors and paramedical staff in basic and advanced life support, the incidence of POCA continues to remain the same. However, the rate of survival after POCA, has improved significantly over the years. POCA is an unpredictable entity but patients with predisposing factors should be monitored closely and appropriate interventions should be performed early all through the perioperative period – from admission to discharge. POCA leading to significant morbidity can be avoided by following protocols and checklists. Effective team dynamics, following life support protocols, thorough evaluation of the patient should be done and all team members should be aware of the events. Events should be documented in the case notes and discharge summary.
Conflicts of interest: NIL
Acknowledgement: NIL
Authors’ contribution: All authors participated in concept, design, literature search, manuscript preparation & review
REFERENCES
- Webb RK, Currie M, Morgan CA, Williamson JA, Mackay P, Russell WJ et al. The Australian Incident Monitoring Study: an analysis of 2000 incident reports. Anaesth Intensive Care. 1993;21(5):520-8.[PubMed] [Free full text]
- Sprung J ,Flick RP, Gleich SJ, Weingarten TN. Perioperative Cardiac Arrests. Signa Vitae 2008;3(2): 8-12.
- Sebbag I, Carmona MJ, Gonzalez MM, Alcântara HM, Lelis RG, Toledo Fde O et al. Frequency of intraoperative cardiac arrest and medium-term survival. Sao Paulo Med J. 2013;131(5):309-14. [PubMed] [Free full text] doi: 10.1590/1516-3180.2013.1315507.
- Siriphuwanun V, Punjasawadwong Y, Lapisatepun W, Charuluxananan S, Uerpairojkit K. Incidence of and factors associated with perioperative cardiac arrest within 24 hours of anaesthesia for emergency surgery. Risk Manag Healthc Policy. 2014;7:155-62.
- Tamdee D, Charuluxananan S, Punjasawadwong Y, Tawichasri C, Kyokong O, Patumanond J et al. Factors related to 24-hour perioperative cardiac arrest in geriatric patients in a Thai university hospital. J Med Assoc Thai. 2009;92(2):198-207. [PubMed]
- Gobbo Braz L, Braz JR, Módolo NS, do Nascimento P, Brushi BA, Raquel de Carvalho L. Perioperative cardiac arrest and its mortality in children. A 9-year survey in a Brazilian tertiary teaching hospital. Paediatr Anaesth. 2006;16(8):860-6. [PubMed] [Free full text] doi: 10.1111/j.1460-9592.2006.01876.x
- Bainbridge D, Martin J, Arango M, Cheng D. Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 2012;380(9847):1075-81. [PubMed] [Free full text] doi: 10.1016/S0140-6736(12)60990-8
- Carlucci MTO, Braz JRC, do Nascimento P, de Carvalho LR, Castiglia YMM, Braz LG. Intraoperative Cardiac Arrest and Mortality in Trauma Patients. A 14-Yr Survey from a Brazilian Tertiary Teaching Hospital. Ang D, ed. PLoS One. 2014;9(2):e90125.[PubMed] [Free full text] doi: 10.1371/journal.pone.0090125
- Kazaure HS, Roman SA, Rosenthal RA, Sosa JA. Cardiac Arrest Among Surgical Patients: An Analysis of Incidence, Patient Characteristics, and Outcomes in ACS-NSQIP. JAMA Surg. 2013;148(1):14-21. [PubMed] [Free full text] doi: 10.1001/jamasurg.2013.671.
- Koga FA1, El Dib R, Wakasugui W, Roça CT, Corrente JE, Braz MG, et al. Anaesthesia-Related and Perioperative Cardiac Arrest in Low- and High-Income Countries: A Systematic Review With Meta-Regression and Proportional Meta-Analysis. Medicine (Baltimore). 2015;94(36):e1465.[PubMed] [Free full text] doi: 10.1097/MD.0000000000001465.
- Nunnally ME , O’Connor MF, Kordylewski H, Westlake B, Dutton RP. The incidence and risk factors for perioperative cardiac arrest observed in the national anaesthesia clinical outcomes registry. Anesth Analg. 2015;120(2):364-70. [PubMed] [Free full text] doi: 10.1213/ANE.0000000000000527.
- JJ , Meltzer EC , Gill HL , Graham AR , Schneider DB , Connolly PH et al. Outcomes and risk factors of cardiac arrest after vascular surgery procedures. J Vasc Surg. 2015;61(1):197-202. [PubMed] [Free full text] doi: 10.1016/j.jvs.2014.06.118.
- Nunes JC, Braz JRC, Oliveira TS, de Carvalho LR, Castiglia YMM, Braz LG. Intraoperative and Anaesthesia-Related Cardiac Arrest and Its Mortality in Older Patients: A 15-Year Survey in a Tertiary Teaching Hospital. PLoS One. 2014;9(8):e104041. [PubMed] [Free full text] doi: 10.1371/journal.pone.0104041.
- Braz LG, Módolo NSP, do Nascimento Jr, Bruschi BAM, Castiglia YMM, Ganem EM et al. Perioperative cardiac arrest: a study of 53 718 anaesthetics over 9 yr from a Brazilian teaching hospital. Br J Anaesth.2006;96(5):569-75.[PubMed] [Free full text] doi: 10.1093/bja/ael065.
- Goswami S, Brady JE, Jordan DA, Li G. Intraoperative cardiac arrests in adults undergoing noncardiac surgery: incidence, risk factors, and survival outcome. Anesthesiology. 2012 ;117(5):1018-26. [PubMed] [Free full text] doi: 10.1097/ALN.0b013e31827005e9.
- Runciman WB, Kluger MT, Morris RW, Paix AD, Watterson LM, Webb R. Crisis management during anaesthesia: the development of an anaesthetic crisis management manual. Qual Saf Health Care. 2005;14(3):e1. [PubMed] [Free full text] doi: 10.1136/qshc.2002.004101.
- Gonzalez LP, Braz JR, Módolo MP, de Carvalho LR, Módolo NS, Braz LG. Pediatric perioperative cardiac arrest and mortality: a study from a tertiary teaching hospital. Pediatr Crit Care Med. 2014;15(9):878-84. [PubMed]
doi: 10.1097/PCC.0000000000000248.
- Bharti N, Batra YK, Kaur H. Paediatric perioperative cardiac arrest and its mortality: database of a 60-month period from a tertiary care paediatric centre. Eur J Anaesthesiol. 2009 ;26(6):490-5. [PubMed]
doi: 10.1097/EJA.0b013e328323dac0.
- Runciman WB, Morris RW, Watterson LM, Williamson JA, Paix AD. Crisis management during anaesthesia: cardiac arrest. Qual Saf Health Care. 2005;14(3):e14.[PubMed] [Free full text] doi: 10.1136/qshc.2002.004473.
- Ellis SJ, Newland MC, Simonson JA, Peters KR, Romberger DJ, Mercer DW et al. Anaesthesia-related cardiac arrest. Anesthesiology. 2014 Apr;120(4):829-38. [PubMed] [Free full text] doi: 10.1097/ALN.0000000000000153.
- Girotra S, Nallamothu BK, Spertus JA, Li Y, Krumholz HM, Chan PS. Trends in Survival After In-Hospital Cardiac Arrest. The New England journal of medicine. 2012;367(20):1912-20. [PubMed] [Free full text] doi: 10.1056/NEJMoa1109148.
http://www.nejm.org/doi/full/10.1056/NEJMoa1109148
- Bayramoglu A, Cakir ZG, Akoz A, Ozogul B, Aslan S, Saritemur M. Patient-Staff Safety Applications: The Evaluation of Blue Code Reports. The Eurasian J Med. 2013;45(3):163-6.[PubMed] [Free full text] doi: 10.5152/eajm.2013.34.
- Huseman KF. Improving code blue response through the use of simulation. J Nurses Staff Dev. 2012;28(3):120-4. [PubMed] doi: 10.1097/NND.0b013e3182551506.
- Kleinman ME, Brennan EE, Goldberger ZD, Swor RA, Terry M, Bobrow BJ et al. Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):S414-35. [PubMed] [Free full text] doi: 10.1161/CIR.0000000000000259.
- Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. 2009;53(2):143-51. [PubMed] [Free full text] doi: 10.1111/j.1399-6576.2008.01717.x.
- Manser T, Harrison TK, Gaba DM, Howard SK. Coordination patterns related to high clinical performance in a simulated anesthetic crisis. Anesth Analg. 2009;108(5):1606-15. [PubMed] doi: 10.1213/ane.0b013e3181981d36.
- Reader TW, Flin R, Mearns K, Cuthbertson BH. Developing a team performance framework for the intensive care unit. Crit Care Med.2009;37(5):1787-93. [PubMed] doi: 10.1097/CCM.0b013e31819f0451.
- Lerner S, Magrane D, Friedman E. Teaching teamwork in medical education. Mt Sinai J Med. 2009;76(4):318-29. [PubMed] [Free full text] doi: 10.1002/msj.20129
- Wacker J, Staender S. The role of the anaesthesiologist in perioperative patient safety. Curr Opin Anaesthesiol. 2014;27(6):649-56. [PubMed] [Free full text] doi: 10.1097/ACO.0b013e3282f70042.
- Adesanya AO, Joshi GP. Hospitalists and anesthesiologists as perioperative physicians: Are their roles complementary? Proc (Bayl Univ Med Cent). 2007;20(2):140-2. [PubMed] [Free full text]
- Gardner-Thorpe J, Love N, Wrightson J, Walsh S, Keeling N. The Value of Modified Early Warning Score (MEWS) in Surgical In-Patients: A Prospective Observational Study. Ann R Coll Surg Engl. 2006;88(6):571-5. [PubMed] [Free full text] doi: 10.1308/003588406X130615
↧
Perfusion science- an international and Pakistani perspective
Hasanat Sharif, Mayera Tufail
Section of Cardiothoracic Surgery, Department of Surgery, Aga Khan University Hospital,
Stadium Road, Karachi (Pakistan).
Correspondence: Dr Hasanat Sharif, Section of Cardiothoracic Surgery, Department of Surgery, Aga Khan University Hospital, Stadium Road, Karachi (Pakistan); Phone: 02134864708; hasanat.sharif@aku.edu
ABSTRACT
Surgery on the heart was considered out of bounds till the invention of the bypass machine in 1953. Since then the significant advancements have been made in the heart lung machine, as it evolved over time. In the initial era, it was operated by operating room technicians or physicians, but with its increased use in the 1960s, a need was soon felt for more trained professionals to operate the machine. Hence, a new breed of professional cardiovascular perfusionists came into existence with formal certification and accreditation.
In United States, Ohio University started formal training of perfusionists in 1969. This was followed by the creation of various organizations to facilitate the accreditation process, such as The American Society of Extra-Corporeal Technology (AmSECT) and American Board of Cardiovascular Perfusion (ABCP). In Europe, The European Board of Cardiovascular Perfusion (EBCP) was founded in 1991 by Cardiovascular Perfusionists, which continued to certify perfusionists. In Pakistan the Pakistan Society of Clinical Perfusionists (PSCP) was formed in 2009, to facilitate former education and certification in perfusion sciences.
Increased demand for quality assurance and to maintain standards of practice in the field of perfusion sciences, has led to the creation of International Consortium for Evidence Based Perfusion (ICEBP). With constant improvements in the heart lung machine to make bypass safer, the perfusionist must be familiar with updated protocols and knowledge to ensure the safety of the patient during cardiac procedures.
Key words: Perfusion; Heart-lung machine
Citation: Sharif H, Tufail M. Perfusion science- an international and Pakistani perspective. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S–
Operating on the heart was thought to be impossible until the invention of the cardio pulmonary bypass in the 1950s. In fact Billroth as President of the World Congress of Surgeons declared in 1896 that any attempt made to suture the heart shall be futile. Ludwig Rehn proved him wrong by successfully performing a repair of a stab wound to the heart.(1) In 1953, Gibbon successfully performed an open heart procedure using a heart lung machine, which worked on the principle of extracorporeal oxygenation; this laid the foundation for modern day techniques used in cardiothoracic surgery.(2, 3) From when it was first invented by Gibbon, the cardiopulmonary bypass techniques have constantly evolved, this not only applies to the apparatus and circuit used for the heart lung machine but also to protocols and standard of work. With the constant advancement of cardiopulmonary bypass, attempts are being made to lessen its less desirable effects. (4) In the 1950s and early 1960s, the operators of the heart lung machine, were often laboratory personnel or physicians. Observation from the laboratory and as well as successive cases in the operating room, imparted necessary skills required for operation of the heart lung machine. With the growth of cardiac surgery and extracorporeal technology in the 1960s, disposable devices and manufactured heart lung machines were born that created a need for more knowledgeable staff.(5, 6) The role of a perfusionist, operating the heart lung machine, came into limelight with the rapid evolution of cardiac surgical services. In the past decade there was a concern regarding the availability of the perfusion man power, thus the occupation of a cardiovascular perfusionist attained a professional status in past 25 years. This was validated by creation of structured processes for the certification of perfusionists and the authorization of perfusionist training programs.(7)
In the United States of America, perfusionist training programs were established to provide training and education to technicians to work in a variety of clinical scenarios, not being limited to the sponsoring institution. The first university sponsored program was created in 1969 at Ohio State University.(8) The training programs become advanced and more structured, The American Society of Extra-Corporeal Technology (AmSECT) started the examination procedure for certification of perfusionists in 1972 led by James Dearing and Louis Toth. The American Board of Cardiovascular Perfusion (ABCP) created in 1975, was an independent organization to assist the process of examination and to oversee the accreditation of perfusion training programs. The Joint Review Committee for Perfusion Education (JRC-PE) was established in 1977, merging the AmSECT and ABCP accreditation principles in the Council on Allied Health Education and Accreditation (CAHEA).(9) CAHEA was replaced by the Commission on Accreditation of Allied Health Education Programs (CAAHEP)in 1994, it sustained providing certification for a structured perfusionist training and education(10) In Europe, perfusion scientists formed the European Board of Cardiovascular Perfusion (EBCP) in 1991. EBCP as an independent entity in perfusion education and training is involved in creating, supervising and maintaining quality of practice and certification of perfusionist training programs as well as authorizing an European certificate of training in perfusion sciences.(11)Trained perfusionists are accredited through a European Certificate on Cardiovascular Perfusion (ECCP).(12)
The first heart lung machine in Pakistan was also operated by a cardiologist in the 1976 at the National Institute for Cardiovascular Diseases (NICVD) in Karachi. Operating room technicians and nurses acquired the skills through on job training and some semi structured programs. The need for patient safety and ensuring quality perfusion was a challenge and to this effect the Pakistan Society of Clinical Perfusionists (PSCP) was formed in 2009. The Dow University of Health Sciences (DUHS) recognized the importance of this highly skilled set of personnel and decided to accredit perfusionists with more than five years’ experience into a Bachelors degree following successful completion of a didactic/interactive course and a final examination. DUHS now has a structured four year bachelors program leading to a BS in clinical perfusion. Other institutions have also developed similar programs. The PSCP is awaiting legislation for Allied Health in the Government of Sindh to commence licensure for perfusionists. The requirements to practice perfusion will require graduation from an accredited program, one year of internship with maintenance of a log of cases. License renewal will depend upon provision of evidence showing a minimum number of cases performed per year and obtaining continuing education credits to keep abreast of the current knowledge in this highly technical field.
Cardiovascular perfusionists have always been keen on maintaining quality standards, mostly in the form of machinery maintenance and data recording. It was primarily developed more as a safety perspective, to reduce variability and improve clinical outcomes.(13,14) The society of perfusion scientists has acknowledged the significance of creating, promoting and implementing perfusion quality practices on the basis of evidence-based medicine. This has led to the birth of the International Consortium for Evidence Based Perfusion (ICEBP).(15)
Perfusion safety is not a secluded component of cardiac surgery, but is multifactorial including machinery and tools, safety devices, conduct of perfusion, surgical technique, awareness, and communication within the boundaries of the operating room. The safety concerns with the heart lung machine during perfusion include oxygenator failures, mechanical failures, electrical failures, massive air embolization, and preventive maintenance.(16,17) Many improvements over the past 45 years have consequently made the cardiopulmonary bypass a safer procedure. This includes advancements from different areas, such as circuit design, engineering and development of the equipment, education and training of cardiovascular perfusionists, implementation of policies, protocols and standards, surgical techniques, and the conduct and management of perfusion.(18) The AmSECT Board of Directors in October 1994, accepted the “Guidelines for Perfusion Practice” and inculcated it into the organization by 1995 in the United States, which provided standards for quality assurance. Safety during cardiopulmonary bypass is accomplished by the development of a critical structured approach, unvarying attention to detail, and relentless quest of quality by the perfusionist and the whole operating team.(19,20)
Conflict of interest: None declared by the authors
Authors’ contribution: HS – Concept, manuscript editing and reviewing; MT – Literature search and manuscript writing
REFERENCES
- Blatchford JW, 3rd, Anderson RW. The evolution of the management of penetrating wounds of the heart. Ann sur. 1985;202(5):615-23..[PubMed] [Free full text]
- Fou AA. John H. Gibbon. The first 20 years of the heart-lung machine. Tex Heart Ins J. 1997;24(1):1-8. [PubMed] [Free full text]
- Cohn LH. Fifty years of open-heart surgery. Circulation. 2003;107(17):2168-70. [PubMed] [Free full text] doi: 10.1161/01.CIR.0000071746.50876.E2
- Passaroni AC, Silva MA, Yoshida WB. Cardiopulmonary bypass: development of John Gibbon’s heart-lung machine. Rev Bras Cir Cardiovasc vol.30 no.2 São José do Rio Preto Mar./Apr. 2015 [Free full text] doi:10.5935/1678-9741.20150021
- Toomasian JM, Searles B, Kurusz M. The evolution of perfusion education in America. Perfusion. 2003;18(4):257-65. [PubMed] [Free full text]
- Hall EF. Mapping the literature of perfusion. Bull Med Libr Assoc. 1999 Jul;87(3):305-11. [PubMed] [Free full text]
- Anderson RP, Nolan SP, Edmunds LH, Jr., Rainer WG, Brott WH. Cardiovascular perfusion: evolution to allied health profession and status 1986. J Thorac Cardiovasc Surg. 1986 Oct;92(4):790-4. [PubMed]
- Plunkett PF. Perfusion education in the USA. Perfusion. 1997;12(4):233-41. Epub 1997/07/01. [PubMed] [Free full text]
- Hill AG, Kurusz M. Perfusion standards and guidelines. Perfusion. 1997;12(4):251-5.. [PubMed][Free full text]
- Stammers AH. Perfusion education in the United States at the turn of the century. J Extra Corpor Technol. 1999;31(3):112-7. [PubMed]
- von Segesser LK. Perfusion education and certification in Europe. Perfusion. 1997;12(4):243-6. [PubMed] [Free full text]
- Merkle F, Mata Forcades MT, Pomar JL, Seeberger M, Wahba A. Statement on the qualification of cardiovascular perfusionists. Interact Cardiovasc Thorac Surg. 2014;18(4):409-10. [PubMed][Free full text] doi: 10.1093/icvts/ivt548
- Stammers AH, Trowbridge CC, Pezzuto J, Casale A. Perfusion quality improvement and the reduction of clinical variability. J Extra Corpor Technol. 2009 Dec;41(4):P48-58. [PubMed] [Free full text]
- Eagle CJ, Davies JM, McCloskey B. An introduction to quality assurance with an application for perfusionists. J Extra Corpor Technol. 1991;23(1):22-5. [PubMed]
- Likosky DS. Integrating evidence-based perfusion into practices: the International Consortium for Evidence-Based Perfusion. J Extra Corpor Technol. 2006;38(4):297-301. [PubMed] [Free full text]
- Palanzo DA. Perfusion safety: defining the problem. Perfusion. 2005;20(4):195-203. [PubMed][Free full text]
- Schabel RK, Berryessa RG, Justison GA, Tyndal CM, Schumann J. Ten common perfusion problems: prevention and treatment protocols. 1987. J Extra Corpor Technol . 2007;39(3):203-9; discussion 1-2. [PubMed]
- Palanzo DA. Perfusion safety: past, present, and future. J Cardiothorac Vasc Anesth. 1997;11(3):383-90. [PubMed] [Free full text]
- Kurusz M. Perfusion safety: new initiatives and enduring principles. Perfusion. 2011;26 Suppl 1:6-14. [PubMed] [Free full text]
- Kurusz M. Standards update on perfusion equipment and practice. Perfusion. 2005;20(4):205-8.
↧
↧
Is majority of requests by anesthesiologists for cardiologist consultation unjustified?
Habib Md Reazaul Karim, MBBS, MD, DNB, IDCCM
Department of Anesthesiology, Critical Care and Pain Medicine. NEIGRIHMS, Shillong-793018 (India)
Correspondence: Department of Anesthesiology, Critical Care and Pain Medicine, North Eastern Indira Gandhi Regional Institute of Health & Medical Sciences (NEIGRIHMS), Mawdiangdiang, Shillong, Meghalaya 793018, (India); Phone: +919612372585 (M); E-mail: drhabibkarim@gmail.com
ABSTRACT
Preoperative consultation of surgical patient by cardiologist is intended to treat an inadequately treated cardiac condition before undergoing surgery. This can yield in terms of new therapy, lead to optimization of the patients’ cardiac comorbidity, impact significantly in terms of perioperative management and potentially reduce postoperative adverse cardiac events. However, judicious use of preoperative consultation request is required both for avoiding unnecessary consultation, investigation and delay in proceeding with surgery as well as cost effective health care delivery. This mini review is aimed at finding the practice patterns of anesthesiologists’ preoperative requests for cardiology consultations. Different clinical situations faced in preoperative evaluation of cardiac patients planned for non-cardiac surgery with regard to the need for preoperative cardiac consultation and a step wise approach for determining the probable need of request is also presented.
Key words: Anesthesia; Analgesia; Referral/consultation, Preoperative; Anesthesiologist; Cardiologist, Non-cardiac surgery
Citation: Karim HMR. Is majority of requests by anesthesiologists for cardiologist consultation unjustified? Anaesth Pain & Intensive Care 2016;20 Suppl 1:S109-S114
Received: 18 September 2016; Reviewed: 10 October 2016; Accepted: 15 October 2016
INTRODUCTION
Preoperative anesthesia check up (consultation) has become an integral part of perioperative care for surgical patients. Observational studies examining the clinical utility of preoperative consultation suggest that it reduces postoperative length of stay.1,2 Many a time anesthesiologist needs to refer the patient to other specialty / super specialty health discipline for consultation and request for cardiologists consultation is also one of them. The purposes of a cardiology consultation are to treat an inadequately treated cardiac condition before surgery, to provide data to use in anesthesia management, and possibly to diagnose a medical condition before surgery which can yield in terms of new therapy impacting perioperative management.3,4
It is well known to health care providers that overuse, underuse and misuse are very important concerns in health care delivery which can lead to patients receiving inappropriate or unnecessary care. 5 Unnecessary referral / consultation even lead to delay in risk stratification / fitness declaration and increases hospital stay.6,7 This mini review is aimed at finding the practice patterns of anesthesiologists’ preoperative requests for cardiology consultations. It is also tried to summarize the justified requests which is expected to help anesthesiologists in rationalizing practices.
PREOPERATIVE CARDIOLOGY CONSULTATION PRACTICES
Preoperative cardiology consultation request is mostly given in patients with known or suspected cardiovascular disease planned for non-cardiac surgery. The common cardiac co morbid diseases leading to consultations are hypertension, coronary artery disease, atrial fibrillation, congestive heart failure etc.8 The precise frequency of preoperative cardiology consultation is difficult to figure out as preoperative consultation services are variable among different hospitals.8 Cardiology consultation is also likely to be same and it may even very among anesthesiologists of same hospital. A study including 13,673 patients undergoing a variety of common procedures (primarily low-risk surgeries) had found that 1.28% of the patients received preoperative cardiology consultation.9 In another observational study with relative smaller participants but including intermediate and high risk surgeries as well have found that the rate of referral by anesthesiologists to cardiologist was 5.33%.6 Similarly, the frequencies of cardiology referral / consultation among all the preoperative medical referrals / consultations are also variable. It was reported as 5.7% in facilities having family physicians to 33 – 40% in facilities without family physician.6,9,10 This indicate that the request of preoperative cardiology consultation is quite prevalent and an area of concern.
The reason for request for preoperative cardiology consultation is also variable. In a retrospective review of cardiology consultations at a university hospital, it was found that 53.47% just asked for an “evaluation,” 39.11% asked for a “clearance,” and 4.46% did not specifically request anything and only 2.97% posed a specific question.11 Incidental and insignificant findings in electrocardiogram and even preoperative risk stratifications have also been shown as reason behind preoperative cardiology consultation.6,12 As a result, the cardiologist often makes broadly inclusive, general remarks (like ‘patient cleared for surgery, patient can be taken up with high-risk, use invasive hemodynamic monitoring etc’) about perioperative management of the patient and may recommend preoperative diagnostic work-up.7,13
ARE ALL PREOPERATIVE CARDIOLOGY CONSULTATION REQUESTS JUSTIFIED?
The value of preoperative cardiology consultation cannot be underestimated, but it is uncertain whether these consultations reach their expected goals.14 Preoperative cardiology consultation also seems to be overused.12,15 Although, previous study has shown that assigning the anesthesiologist with the responsibilities of deciding which patients need further evaluation has been associated with a 73% decrease in preoperative consultations,16 anesthesiologists are still asking inappropriate / unnecessary cardiology consultations.6 In a prospective observational study, it was found that 3 out of 4 cardiology referral (75%) was not required / inappropriate.6
Examining the cardiology consultation requests in 712 patients scheduled for elective surgery, Aslanger et al. found that the cardiologists revealed an abnormality in 67.8% and recommended further work up in 58.7% of the patients. However, they contributed to the clinical course in only 36.9%. It was also found that when the algorithm was applied to ‘routine pre-operative evaluation’ requests lacking a specific question, only 7.6% of these consultation requests required further investigation.15 Another study evaluating the indication of the requests for preoperative cardiac consultation for in patients undergoing non-cardiac surgery found that only 26.5% of the requests were according to the 2009 ACC/AHA guidelines.17
A study with 100 patients of positive cardiac history and symptoms and signs suggestive of cardiac disease, screened by anesthetist and referred to single cardiologist for cardiac risk stratification and further treatment (if required) found that only 16% were identified as high risks and only one patient needed further intervention; even though 55% patients had cardiac co morbidities.12 Evaluating the effect of preoperative cardiology consultation prior to elective aortic aneurysm repair on patient morbidity, it was found that although those patients who had a preoperative cardiology consult were at greater risk, there were no decrease in postoperative cardiac complications.18 These clearly indicate that requesting a cardiology consultation in all patients having cardiac co morbidities / undergoing major and high risk surgeries does not change anesthetic management and postoperative outcome much and thus preoperative consultation in all patients cannot be accepted or justified.
WHEN TO REQUEST A CARDIOLOGY CONSULTATION?
The preoperative request for consultation by other specialty should probably be governed by the same rule as for preoperative investigations and should be asked if only it is going to change anesthetic management of the patient. It is recommended that the preoperative investigation should be based on the history, physical examination, perioperative risk assessment, and clinical judgment,19 anesthesiologist should ask for cardiology or other specialty consultation based on the patients history, physical examination, functional capacity (as judged clinically by metabolic equivalents of task), co morbid conditions and type of the indexed surgery and its risk estimate. European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA) recommend a multidisciplinary expert team for pre-operative evaluation of patients with known or high risk of cardiac disease undergoing high-risk non-cardiac surgery.20 In their guideline ESC and ESA also recommends regarding cardiovascular assessment and management of cardiac patients planned for non-cardiac surgery.20
Literature has clearly shown that in terms of perioperative management—other than the management of perioperative acute coronary syndromes—the cardiology consultation has little to add and even non-cardiac surgery can be done in patients with severe aortic stenosis.4,13 Therefore the decision for preoperative cardiac assessment or cardiology consultation probably can be best derived from the stepwise approach to perioperative cardiac assessment and treatment algorithm for coronary artier disease provided by American college of cardiology (ACC) and American heart association (AHA).21 It is clear from the ESC/ESA and ACC/AHA guideline that the further cardiac evaluation of patients planned for non-cardiac surgery should be based on cardiac conditions, type and urgency of the surgery, estimated perioperative risk of major adverse cardiac events on the basis of the combined clinical/surgical risk, functional capacity etc.20, 21 Active cardiac conditions and clinical cardiac risk factors are presented in Boxes 1 and 2 respectively.20,22

A suggested stepwise algorithm for determining the need of preoperative cardiology consultation request Figure 1. As the reasons for request of preoperative cardiology consultations differ from hospital to hospital and even anesthesiologist to anesthesiologist, possible clinical situations with suggested preoperative cardiologic consultation requests for elective non-cardiac surgery are presented in Table 1 based on the current literature, recommendations and guidelines.
Figure 1: Stepwise flow chart for preoperative cardiac consultation request for elective surgery (MACE- Major adverse cardiac events, METs- Metabolic equivalent of Tasks) adapted from 2014 ACC/AHA and 2014 ESC/ESA guideline for cardiac evaluation for non-cardiac surgery.
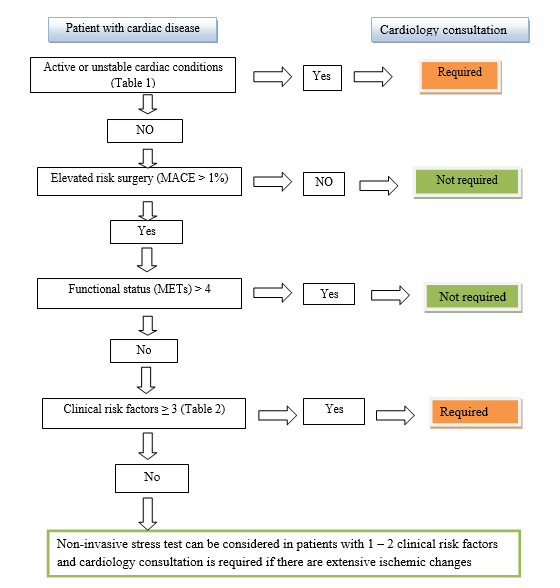
It is very much clear that despite having evidence based guidelines inappropriate practices are still well prevalent. The maximum benefit of these recommendations and guidelines probably can be obtained by following and developing institutional / national adapted protocols.23 In an era when anesthesiologists are claiming and considered as perioperative physicians, profession demands behavioral changes of anesthesiologists as well over and above the name change.13 The post graduate training / residency program in anesthesiology should also be adapted accordingly and probably a posting in cardiology and internal medicine is also required for such change.
Table 1: Possible clinical situations with suggested preoperative cardiologist consultation request for elective non-cardiac surgery. (Prepared from 2014 ESC/ESA and 2014 ACC/AHA guideline for non-cardiac surgery and Parks review)3,20,21
| Clinical situations | Comments with regard to cardiac consultation |
| Controlled arterial Hypertension
Uncontrolled arterial Hypertension
Malignant arterial Hypertension |
Proceed with surgery
Proceed with surgery if blood pressure < 180 / 110 mmHg in adults. Consider escalation of dose. If uncontrolled with 3 drugs, request for cardiology consultation Postpone surgery and request cardiology consultation |
| Known case of Coronary Artery Disease, Heart Failure
Acute / severe / decompensated Stable / optimized / chronic |
Postpone surgery and refer to cardiologist for treating / optimization of cardiac condition
Proceed with surgery with risk stratification and reduction strategies / medication continued |
| Unexplained, new onset dyspnea / chest pain | Request cardiologist consultation for ruling out /treating (if required) of active cardiac conditions |
| Post Percutaneous Transluminal Coronary Angioplasty / Coronary Artery Bypass Graft within 6 years | With asymptomatic stable / improved condition and good METs can be proceeded for surgery |
| Severe aortic stenosis symptomatic
Severe aortic stenosis asymptomatic
Severe Mitral stenosis Regurgitant valvular heart disease |
Postpone high risk surgery, request consultation of cardiology and cardiac surgeon for valve replacement / balloon valvuloplasty
Proceed with low and intermediate risk surgery. Request consultation if planned for high risk surgery If with symptoms of severe pulmonary hypertension, postpone surgery and request cardiology consultation Request consultation if there is symptoms and signs of severe heart failure / left ventricular dysfunction |
| Patients with prosthetic valve | Modify anticoagulation and proceed for surgery unless there is valve / ventricular dysfunction |
| Severe pulmonary arterial hypertension (PAH) | Request cardiology consultation for an optimized treatment regimen and proceed with PAH- specific medication continued |
| Arrhythmias / Dysrhythmia | Request consultation if acute, symptomatic and significant arrhythmias / or pacemaker is indicated before proceeding for surgery.
Premature beats, fascicular blocks, bradycardia without symptoms, fist degree and second degree Mobitz type I do not need request for cardiology consultation and can be proceed with surgery |
| Peripheral arterial disease | Request consultation if > 2 clinical risk factors are present |
| Patients with unknown functional capacity | Exercise stress testing may be reasonable to perform for major / elevated risk surgery |
| Drugs (Anticoagulant, beta blocker, anti-hypertensive, statin etc) | Manage as per guideline / recommendations. If beta blocker is indicated but patient is not amenable, request for cardiology consultation |
| Investigations (electrocardiogram, echocardiography, stress test, cardiopulmonary exercise testing etc) | Ask for the investigation if indicated. Cardiology consultation request is required only if the abnormality mandates active cardiac management before proceeding with surgery for better outcome |
| Risk stratification, Clearance | No. It is the anesthesiologists job / duty |
| Pacemaker in situ | Proceed as per recommendation. Go through documents |
CONCLUSION
Mere presence of a cardiovascular disease does not warrant preoperative cardiology consultation. Stable cardiovascular disease including asymptomatic coronary artery disease patient can undergo non-cardiac surgery without preoperative cardiology consultation with appropriate perioperative medication and monitoring by anesthesiologist. A consultation request for risk stratification, clearance for surgery should not be done rather a request for preoperative cardiology consultation should be done if it is going to change the course of perioperative management.
Acknowledgement: None
Competing Interest: None
Author contribution: This manuscript has been prepared by the author, and he accepts full responsibility for the correctness of the material given.
REFERENCES
- Wijeysundera DN, Austin PC, Beattie WS, Hux JE, Laupacis A. A population-based study of anesthesia consultation before major noncardiac surgery. Arch Intern Med 2009;169:595-602.
[PubMed] [Free full text] doi:10.1001/archinternmed.2009.3
- Chan FW, Wong F, Cheung YS, Chui PT, Lai PB. Utility of a preoperative assessment clinic in a tertiary care hospital. Hong Kong Med J 2011;17:441-5.
- Katz RI, Barnhart JM, Ho G, Hersch D, Dayan SS, Keehn L. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg 1998;87:830–6.
- Park KW. Preoperative cardiology consultation. Anesthesiology 2003;98:754–62.
- Lambrinos, A. Preoperative consultations: a rapid review. Toronto: Health Quality Ontario; 2014 March [cited 2016 Sept 17]:p1-19. [Free full text]
- Karim HM, Yunus M, Bhattacharyya P. An observational cohort study on pre-operative investigations and referrals: How far are we following recommendations? Indian J Anaesth 2016;60:552-9. [PubMed] [Free full text] doi:10.4103/0019-5049.187783
- Braham RL, Ron A, Ruchlin HS, Hollenberg JP, Pompei P, Charlson ME. Diagnostic test restraint and the specialty consultation. J Gen Int Med 1990;5:95–103.
- Wijeysundera DN, Austin PC, Beattie WS, Hux JE, Laupacis A. Variation in the practice of preoperative medical consultation for major elective noncardiac surgery: a population-based study. Anesthesiology 2012;116:25-34.
[PubMed] doi: 10.1097/ALN.0b013e31823cfc03
- Thilen SR, Bryson CL, Reid RJ, Wijeysundera DN, Weaver EM, Treggiari MM. Patterns of Preoperative Consultation and Surgical Specialty in an Integrated Healthcare System. Anesthesiology 2013;118:1028-37.
[PubMed] [Free full text] doi: 10.1097/ALN.0b013e31828ea68a
- Paik H, Lim C-W, Ryu H-G. Characteristics and effectiveness of preoperative consultations in a tertiary hospital. Korean J Anesthesiol 2013;65(6 Suppl):S4-S5.
[PubMed] [Free full text] doi:10.4097/kjae.2013.65.6S.S4
- Kleinman B, Czinn E, Shah K, Sobotka PA, Rao TK: The value to the anesthesia-surgical care team of the preoperative cardiac consultation. J Cardiothor Anesth 1989;3:682–7.
- Malik MN, Fatima N, Farah, Memon MI. Preoperative Anesthesia Referrals to Cardiology and Outcome in a Tertiary care hospital. Ann Pak Inst Med Sci 2014; 10(2):89-92.
- Kleinman B. Preoperative Cardiology Consultation: How Helpful Is It? Anesthesiology 2003;99:1240. [PubMed]
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. Circulation 2009;120:e169-276. [PubMed] [Free full text] doi:10.1161/CIRCULATIONAHA.109.192690
- Aslanger E, Altun I, Guz G, Kiraslan O, Polat N, Golcuk E, Oflaz H. The preoperative cardiology consultation: goal settings and great expectations. Acta Cardiol 2011;66:447-52. [PubMed] [Free full text] doi:10.2143/AC.66.4.2126592
- Fischer SP. Development and effectiveness of an anesthesia preoperative evaluation clinic in a teaching hospital. Anesthesiology 1996;85:196-206. [PubMed] [Free full text]
- Antonelli D, Jabaren M, Turgeman Y. Requests for preoperative cardiology consultation for patients undergoing non cardiac surgery. Harefuah 2014;153:515-7, 559-60. Hebrew. [PubMed]
- Eliassen AM, Davis FM, Phillips AR, Robinson AB, Henke PK. Effect of Preoperative Cardiology Specialty Consultation Prior to Elective Aortic Aneurysm Repair on Patient Morbidity. J Vasc Surg 2015;61 (6 suppl):S58. [Free full text] doi: 10.1016/j.jvs.2015.04.106.
- Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative Testing Before Noncardiac Surgery: Guidelines and Recommendations. Am Fam Physician 2013;87:414-8.
- Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J 2014;35:2383-431. [PubMed] [Free full text] doi:10.1093/eurheartj/ehu282
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;130:2215-45. [PubMed] [Free full text] doi:10.1161/CIR.0000000000000105
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, et al. 2007 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2007;116:418-99. [PubMed] [Free full text]
- Yunus M, Karim HM, Dey S. What is new in guidelines on preoperative tests and how to maximize benefit out of different guidelines? Archives Medical Review Journal. Forthcoming 2017;26:
↧
Off‐pump coronary artery bypass surgery
Amarja Sachin Nagre, MD, DM, FCA*
*Dr Amarja Sachin Nagre, Assistant Professor, N-6, Cidco, Aurangabad, Maharashtra 431003, (India)
The rationale behind development of off pump coronary artery bypass (OPCAB) surgery is avoidance of CPB related complications in addition to other advantages like decrease in postoperative neurocognitive and renal dysfunction. It is associated with decrease in postoperative morbidity, accelerates recovery and leads to early ICU and hospital discharge. Ultrafast tracking and awake OPCAB under high thoracic epidural are significant advances. Anesthetic management of OPCAB patients is targeted to maintain hemodynamic stability and prevent myocardial ischemia during coronary grafting. Meticulous preanesthetic assessment, monitoring, titrated usage of induction agents, balanced anesthetic technique and vigilance during grafting is the essence of anesthetic management during OPCAB.
Octopus Tissue Stabilizer minimizes the motion of the small area of the heart where the bypass graft is to be attached while the rest of the heart continues to beat normally. Starfish is the positioner attached at the cardiac apex which locks the longitudinal axis of the heart, thereby allowing access to coronary vessels of the lateral and posterior walls. Intracoronary shunts secure the blood flow through the coronary vessels during the procedure.
Left anterior descending (LAD) grafting (Figure 1) involves ‘displacement’ of the heart forward and superior to facilitate LAD anastomosis by placing pericardial stay sutures and mops underneath the heart.
Left circumflex artery (LCX) grafting (Figure 2) is the most critical anastomosis as exposure is difficult which demands lifting the heart and placing it in an unphysiologic position called as ‘verticalization’, achieved by displacing heart to right side. Placing Octopus stabilizer system leads to compression of right ventricle and distortion of the tricuspid and mitral annuli. Steps to combat hypotension and hypoperfusion are opening of right pleura to accommodate RV, application of Starfish apical suction device, trendelenburg position, use of vasopressors and inotropes, judicious volume expansion as excess volume administration causes increase in left ventricular end diastolic volume (LVEDV) and hence LVEDP. This leads to decrease in coronary perfusion pressure.
Right coronary artery (RCA) grafting (Figures 3 & 4) may result in severe ischemia during clamping of RCA and complete atrioventricular block attributable to interruption of the blood flow in the AV node artery.(9)
Ultrafast tracking of Anesthesia (UFTA): The term ultrafast tracking includes shortening of prolonged postoperative ventilatory support, or even immediate extubation, reducing ICU stay and postoperative monitoring, and early discharge.13 Concerns about UFTA with early extubation include increased respiratory and cardiac workload causing myocardial ischemia, reintubation, hypothermia, shivering, inadequate analgesia, and perhaps mortality. Mediastinal bleeding requiring reexploration is a potential problem in cardiac surgery wherein a secured airway is desired. Benefits of early extubation after cardiac surgery are reduced lung trauma with decrease in the stress and discomfort of endotracheal tube suctioning and weaning from ventilation. Sedative drugs and ventilator disposables requirement is lessened. Patients are transferred early to lower dependency units. Nursing staff required to manage each patient is less. Early extubation saves cost through decreasing the usage of oxygen, ABG sampling, suction catheters, gloves, power consumption and manpower requirement.
References
- Lazar HL. Should off-pump coronary artery bypass grafting be abandoned?. Circulation. 2013 Jul 23;128(4):406-13. [PubMed] [Free full text] doi:1161/CIRCULATIONAHA.113.003388
- Sellke FW, DiMaio JM, Caplan LR, Ferguson TB, Gardner TJ, Hiratzka LF, Isselbacher EM, Lytle BW, Mack MJ, Murkin JM, Robbins RC. Comparing On-Pump and Off-Pump Coronary Artery Bypass Grafting Numerous Studies but Few Conclusions: A Scientific Statement From the American Heart Association Council on Cardiovascular Surgery and Anesthesia in Collaboration With the Interdisciplinary Working Group on Quality of Care and Outcomes Research. Circulation. 2005 May 31;111(21):2858-64. [PubMed] [Free full text]
- Chassot PG, Van der Linden P, Zaugg M, Mueller XM, Spahn DR. Off‐pump coronary artery bypass surgery: physiology and anaesthetic management. Br J Anaesth. 2004 Mar;92(3):400-13. [PubMed] [Free full text] doi:1093/bja/aeh064
- Kiessling AH, Huneke P, Reyher C, Bingold T, Zierer A, Moritz A. Risk factor
analysis for fast track protocol failure. J Cardiothorac Surg. 2013 Mar 15;8:47. [PubMed] [Free full text] doi: 10.1186/1749-8090-8-47.

Figure 1: Left anterior descending (LAD) grafting. Intracoronary shunt kept outside the anastomosis for demonstration

Figure 2: Left circumflex artery (LCX) grafting. Note the ‘verticalization’ of the heart.

Figure 3: Right coronary artery (RCA) grafting.

Figure 4: Right coronary artery (RCA) anastomosis.

With Prof Octavio Alfieri- the biggest name in Mitral Valve repair and Alfieri stitch is his contribution.. He demonstrated the same and stressed the importance of perioperative TEE and importance in avoiding SAM
(Courtesy: Vikram Basappanavar)
↧
Anesthetic management of a patient with dilated cardiomyopathy and end stage renal disease
Meena Singh, MD1, Madhu Dayal, MD2
1Assistant Professor, Department of Anesthesia & Intensive Care, Netaji Subhash Chandra Bose (NSCB) Medical College, Jabalpur, Madhya Pradesh 482001, (India)
2Specialist, Department of Anesthesia & Intensive Care, Vardhman Mahavir Medical College (VMMC) and Safdarjung Hospital, New Delhi, (India); Email: dr.madhudayal@gmail.com
Correspondence: Dr. Meena Singh, House No. 127, Nehru Nagar, Opposite Medical College, Jabalpur, MP-282003 (India); Cell: 09891583499; Ph: 0761-2673199; E-mail: dr.meenasingh2010@gmail.com
ABSTRACT
Cardiovascular disease is the leading cause of mortality among patients with end stage kidney disease (ESKD). Left ventricular hypertrophy (LVH) and left ventricular dilation (LVD) are independent risk factors for mortality and make the management of a patient with dilated cardiomyopathy (DCM) and ESKD stage 5. undergoing noncardiac surgery is a real challenging task as the perioperative course may be complicated by cardiac arrhythmias or cardiac failure at any time and associated with high perioperative morbidity and mortality. An adequate knowledge of the pathophysiology of these diseases and treatment modalities is essential to manage these cases successfully. Meticulous planning is the key to success. We stress that adequate preoperative preparation and a planned anesthesia leads to a successful management of dilated cardiomyopathy with ESKD.
Key words: Cardiomyopathy, Dilated; End stage kidney disease; Anesthesia; General anesthesia management
Citation: Singh M, Dayal M. Anesthetic management of a patient with dilated cardiomyopathy and end stage renal disease. Anaesth Pain & Intensive Care 2016;20(4):471-473
Received: 19 Mar 2016; Reviewed: 10 May, 12 Jun 2016; Corrected: 12, 19 Nov 2016; Accepted: 4 Dec 2016
INTRODUCTION
Patients with ESKD are at extreme cardiovascular risk. At least half of all patients starting dialysis therapy have overt cardiovascular disease such as new onset heart failure, peripheral vascular disease, ischemic heart disease and stroke. High level exposure to traditional risk factors such as smoking and dyslipidemia, hemodynamic overload and metabolic factors related to uremia all likely may play a role.1 Cardiovascular disease accounts for over 40% of deaths in ESKD patients.2 In general patients with even mild chronic kidney disease have greater burden of incident CVD compared with similar age control.3There are various cardiovascular abnormalities that are commonly encountered in patients with chronic kidney disease or ESRD; these include LVH, LV dilatation, and LV systolic and diastolic dysfunction.4 We want to highlight the points related to anesthesia concern by reporting this case with dilated cardiomyopathy and ESKD undergoing an emergency laparotomy for strangulated inguinal hernia.
CASE REPORT
A 33 year old male, weighing 55 kg, a known case of DCM with ESKD on multiple hemodialysis since 2 years, presented for emergency laparotomy with diagnosis of strangulated hernia. He had undergone dialysis 3 days back and was on following medications; torsemide 100 mg, clinidipine 10 mg, moxonidine 0.3 mg, losartan 50 mg and prazocin 10 mg. On pre-anesthesia checkup his heart rate (HR) was 170/min and blood pressure (BP) was 202/140 mmHg. His RR was 25-30/min. Bilateral basal crepitations were present on systemic examination. Fresh ABG’s showed PO2 83.1 mmHg, PCO2 34.3 mmHg, pH 7.44, HCO3 22.9 mEq/L, and SaO2 96.6%. Arterio-venous fistula was seen on left cubital fossa. Preoperative investigations were; Hb 9.7 g/dl, TLC 10,000 /mm3, Platelet count 2,62000 /mm3, RBS 88 mg/dl, serum Na+135 mEq/L, K+ 4.2 mEq/L, Ca2+ 8.5 mg/dl, coagulation profile within normal limits, BU 143, creatinine 13.4 and creatinine clearance was <15 ml/min.
12 Lead ECG showed sinus tachycardia and severe LVH. A 2D-echo showed hypertensive heart disease, cardiomyopathy, global left ventricular hypokinesia, severe concentric hypertrophy, severe left ventricular systolic dysfunction, and an ejection fraction 25-30 %. Left atrium and ventricles were dilated. Chest x-ray revealed cardiomegaly with CT ratio 0.52 and bilateral pleural effusion. The patient’s abdominal USG showed small and scarred kidneys, moderate amount of ascites with component of cystitis. Cardiology and nephrology consultations were taken. High risk consent and consent for post-operative ICU care was obtained. With the intention to optimize our patient preoperatively, inj fentanyl and inj metoprolol were administered IV slowly. After 10 min of administering drugs HR and BP came down to 128/min and 150/100 mmHg respectively.
In OR standard monitors were attached. Under local anesthesia, an arterial line (right radial) and central venous pressure (CVP) line (in right internal jugular vein) were passed. Antiarrhythmic drugs (amiodarone, digoxin, lignocaine), vasodilators, vasopressors (adrenaline and noradrenaline) and dopamine were kept ready along with stand-by defibrillator. After preoxygenation with 100% oxygen for 3 min, general anesthesia was induced with a repeat dose of fentanyl 50 µg, etomidate 15 mg and atracurium 25 mg. Lignocaine 60 mg was used to blunt intubation response. Trachea was intubated with cuffed ETT 8 mm ID. General anesthesia was maintained with O2/N2O, isoflurane and atracurium. HR, ECG, invasive BP, SpO2, EtCO2, CVP, urine output, temperature, SE and ABG’s were monitored and corrected. Surgery lasted for 60 min with a total blood loss of 350 ml. Metoprolol 2 mg (in graded dose of 1 mg) was used to keep heart rate below 100/min. Nitroglycerine (NTG) infusion was titrated (0.5-2 µg/kg/min) to maintain blood pressure around 140/90 mmHg and intra-operative CVP was kept between 7-10 cmH2O with 0.9% normal saline and one unit of packed red blood cell. Urine output was 50 ml. Paracetamol 1 gm was given IV for postoperative pain relief. Blood pressure remained stable on NTG infusion. After completion of surgery, patient was shifted to intensive care unit for elective ventilation and monitoring with further cardiologic evaluation. In ICU patient was given fluids guided by CVP and NTG infusion was titrated and stopped gradually. Trachea was extubated after 48 h, then he was shifted to HDU of surgery unit and subsequently discharged on twice weekly hemodialysis.
DISCUSSION
The aim of this case report is to provide brief review of the management goals with particular attention given on the management of perioperative arrhythmias and prevent further complications intended to get a good outcome. In the absence of intrinsic heart disease, LV enlargement is most probably attributable to chronic volume/flow overload associated with 3 principal factors: Anemia, the presence of arteriovenous shunts and sodium water retension.5 Along with these factors, hypertension which is leading cause of LVH6, is also a common and challenging entity, for anesthesiologist to manage. All these findings are present in our patient, so particular emphasis was given on: careful induction of general anesthesia, avoidance of myocardial depression, maintain normovolemia and normothermia, reduction in ventricular preload and afterload, avoidance of intra-operative tachycardia and hypertension, avoidance of hypoxia, hypercarbia and metabolic acidosis, avoidance of nephrotoxic drugs, maintenance of adequate renal perfusion pressure, avoidance of drugs requiring renal metabolism for termination of action which might worsen the clinical condition of the patient. For induction of general anesthesia inj etomidate had been chosen as it is like ketamine and narcotics having minimal depressive effects on cardiac function. During maintenance of anesthesia, the dose dependent direct myocardial depression produced by volatile anesthetics must be considered. It is recommended that fluid therapy and pharmacological management be guided by the use of pulmonary artery catheter and determination of cardiac filling pressure but this facility was not available in our hospital during emergency services, so we relied on CVP that was monitored throughout the perioperative period to avoid volume overload. We used NTG infusion mainly to reduce afterload, it is a venodilator at low doses and arterial dilator at a high dose, lowering intracardiac pressure and alleviating pulmonary congestion. It also dilates coronary arteries making it useful in patients with heart failure and myocardial infarction (MI). Lignocaine, amiodarone and/or defibrillation must be used to treat any arrhythmias if required7, which usually occur due to reduced levels of K+ and Mg2+ that should be assessed and corrected pre-operatively. For this reason we kept these drugs and defibrillator ready by the side.
Patients with CKD surgical stimulation my produce undesirable increases in heart rate, which may be treated with beta-antagonists such as metoprolol or esmolol, keeping in mind the potential for these drugs to cause cardiac depression. Adequate oxygenation and ventilation were closely monitored with SpO2 and EtCO2. Metabolic acidosis is very common in CKD patients but initiation of dialysis typically results in improvement of metabolic acidosis due to addition of base load delivered in dialysate. As we had already put an arterial line, ABG monitoring during ICU stay became easy. Increased sympathetic nervous system activity is form of tachycardia and hypertension is present in the vast majority of these patients and plays a key role in progressive deterioration of renal function and in the exceedingly high rate of cardiovascular events, which represent the primary cause of morbidity and mortality in this patient group.
Anemia (Hb levels 6-12 g/dl) is an independent predictor of mortality in dialysis patients,1 therefore, a Hb level equivalent to 13-14 g/dl has been recommended.8 Cardiac output may be improved by inotropes, biventricular synchronized pacing or an aortic balloon pump.
Regional anesthesia for example epidural anesthesia, may be an alternative to general anesthesia in selected patients. Clinical experience is limited, however and caution is indicated to avoid an abrupt onset of blockade of sympathetic nervous system innervation. Since the patient’s general condition was very poor with signs of pulmonary hypertension, uncontrolled hypertension and tachycardia, we relied on general anesthesia. With meticulous monitoring, judicious use of required drugs and proper knowledge, general anesthesia can be induced safely with improved outcome.
CONCLUSION
During perioperative period, various important factors should be keep in mind before giving anesthesia to a patient with DCM complicated with ESKD; therefore, we must be aware of pathophysiology, signs and symptoms, diagnostic evaluations and treatment modalities to manage these cases successfully.
Conflicts of interests: None
Authors’ contribution: Both authors took equal part in the management of the case and the manuscript preparation.
REFERENCES
- Foley RN. Clinical epidemiology of cardiac disease in dialysis patients: left ventricular hypertrophy, ischemic heart disease and cardiac failure. Semin Dial. 2003 Mar-Apr;16(2):111-7. [PubMed]
- United States Renal Data System. USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institute of Health, National Institute of Diabetes, Digestive and Kidney Diseases, Bethesda, MD 2013. [Free full text]
- Go AS, Chretow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004 Sep 23;351(13):1296-1305. [PubMed] [Free full text]
- Jardine AG, McLaughlin K. Cardiovascular complications of renal disease. Heart. 2001 Oct;86(4):459-466. [PubMed] [Free full text]
- London G M. Left ventricular alterations and end-stage renal disease. Nephrol Dial Transplant. 2002;17 Supl 1:29–36. [PubMed] [Free full text]
- Siedlecki A, Muslin AJ. Left ventricular hypertrophy in the setting of chronic kidney disease—mechanisms and treatment. US Nephrol. 2008;3:40–42.
- Thiagarajah PH, Thiagarajah S, Frost E. Anaesthetic considerations in patients with cardiomyopathies– a review. Middle East J Anesthesiol. 2009 Oct;20(3):347-54 [PubMed]
- Sharma R, Francis DP, Pitt B, Poole-Wilson PA, Coats AJ, Anker SD. Hemoglobin predicts survival in patients with chronic heart failure: a sub study of the ELITE II trial. Eur Heart J. 2004 Jun;25(12):1021-8. [PubMed] [Free full text]
↧
REAL STORIES FROM ICU : The senior doctor
Muhammad Haroon
Consultant intensivist, Maxhealth Hospital, Office No. 2/101, G-8 Markaz, Islamabad (Pakistan); Phone: +92 51 809 4760 ; E-mail: haroonoptimist@gmail.com
“We have paid so much amount of money for our patient; if he dies here, we will break the bones of that senior doctor who is not coming to see the patient”, said an aggressive attendant.
“Please calm down, he is busy and operating a critical accident victim with multiple injuries” said ICU medical officer.
“We don’t care about what he is doing. We want him here in next 10 minutes otherwise we are going to turn your hospital upside down.” said another attendant.
Dr S called senior surgeon again. An assistant replied that the surgeon was stuck in an emergent surgery and couldn’t reply.
Meanwhile, the professor of anesthesiology arrived at the scene and asked the doctor what was going on. Why so many people have surrounded the ICU and shouting. What’s wrong with their patient?” He asked. “Sir, their patient has sepsis, MODS, complicated diabetes, stroke and infected bed sores. Family is concerned about his high grade fever, which is not responding to medicines and cold sponging. The physician I/C has advised surgical consultation for debridement of bed sores as it may bring down his fever” told the MO.
After few minutes both doctors entered the waiting hall and were immediately surrounded by angry attendants.
“Here is our head of ICU, Professor I. He has been specially called by hospital admin to address your issues”, said the MO.
“Our patient needs urgent surgery for bed sores and if it’s not done immediately we are going to ….”, started a youthful attendant.
“Yes I agree with you. He needs urgent surgery and we are shifting him straight away to the operating room. The head of surgery and transplantation departments are here with their staff. Your patient has severe anemia and surgery will cause a lot of blood loss. Please go and immediately arrange 8 pints of blood, 12 pints of plasma and 8 pints of platelets.” said the professor.
“This is the responsibility of the hospital to provide blood.” said a family member.
“Yes my dear we will do a complete screening and will process the blood in our blood bank but our bank is short of group O-positive blood and all of you have to donate at least one pint each for your patient. Don’t worry, nothing will happen to the donors. Those below 10 years will donate half pint.” Said the professor and went back to OT.
The attendants cooled down and looked sadly at each other. They started dispersing. The younger boys disappeared from the scene first. The professor re-entered and announced that both kidneys of patient have failed and he urgently needs a kidney to survive. So all attendants must get HLA typing to match kidney for donation.
After 30 minutes of the announcement, the MO entered anesthesia room with a smile on his face, “Sir, only the patient’s wife and son are left outside and they are asking if they could purchase blood and kidney from somewhere as they are unable to arrange it”.
↧
↧
Comparison of postoperative analgesia with 0.8 mg and 1.6 mg intrathecal nalbuphine; a randomized controlled trial
Prasanna Vadhanan1 Kiruthika Balakrishnan 1
Department of Anesthesiology, Vinayaka Missions Medical College and Hospitals (VMMC), Karaikal 609 609, Pondicherry, (India)
Correspondence: Dr. Prasanna Vadhanan, No 6, P&T Nagar, Mayiladuthurai -609609 (India); Phone: +919486489690; E-mail: vadhanan.prasanna@gmail.com
ABSTRACT:
Background & Objectives: Intrathecal opioids provide an easy and efficient method of prolonging postoperative analgesia due to its action on the spinal opioid receptors. Nalbuphine is a mixed opioid agonist – antagonist which has better side effect profile than morphine. It is easily available in India without a need for narcotics license. The optimal dose of nalbuphine as an adjuvant to intrathecal bupivacaine is not known, as the availability of other narcotics, e.g. fentanyl, sufentanyl etc., in the West has diminished the need to use, and thus to research partial opioids like nalbuphine.
The aim of our study was to compare the duration of postoperative analgesia with 0.8 mg and 1.6 mg of nalbuphine when used as an additive with 0.5% hyperbaric bupivacaine in patients undergoing lower abdominal and lower limb surgeries.
Methodology: 66 patients undergoing various lower abdominal and lower limb surgeries were randomized into 2 groups and received either 0.8 mg or 1.6 mg intrathecal nalbuphine with 3.2 ml of 0.5% hyperbaric bupivacaine. The duration of postoperative analgesia, hemodynamic stability and incidence of adverse effects were noted.
Results: The mean duration of postoperative analgesia in 0.8 mg and 1.6 mg group were 247 ± 12 and 239 ± 10 min respectively (p = 0.007). The incidence of bradycardia was more in 1.6 mg group but did not reach statistical significance. The inability of the higher dose to achieve longer analgesia might be due to a ceiling effect and anti-analgesic actions of nalbuphine.
Conclusion: A dose of 0.8mg of nalbuphine as an intrathecal adjuvant seems to be optimal for providing prolonged postoperative analgesia with minimal side effects.
Key words: Nalbuphine; Postoperative pain; Anesthesia, Spinal; Analgesia
Citation: Comparison of postoperative analgesia with 0.8 mg and 1.6 mg intrathecal nalbuphine; a randomized controlled trial. Anaesth Pain & Intensive Care 2017;21(1):37-43
Received: 25 Sep 2016; Reviewed: 14 Feb 2017; Corrected & Accepted: 11 Mar 2017
INTRODUCTION:
Postoperative pain is associated with lot of negative outcomes like cardiovascular events, poor ventilation, impaired wound healing and poor patient satisfaction. Pain is usually moderate to severe in the immediate postoperative period as the patient recovers from anesthesia. The “First pain” is usually sharp, pricking and localized to the surgical site and is mediated by nociceptors. 1 Central sensitization can occur during periods of exacerbation of acute pain. Adequate analgesia during this period can prevent the negative outcomes and help in early mobilization. Still postoperative pain is undertreated and there is a long way to go towards this objective.2 Intrathecal opioids as an adjuvant to local anesthetics provide an easy and effective way of pain control in the immediate postoperative period. The main reservations against opioids are concerns about side effects like respiratory depression, sedation and availability. Nalbuphine is a semi-synthetic opioid agonist-antagonist analgesic of the phenanthrene series. The drug has been shown to have lesser propensity to cause respiratory depression when compared to morphine in several studies including those in pregnant population.3
The intrathecal dosage of the drug varies from 0.4 to 2.0 mg .4,5 The optimal dose of nalbuphine for this purpose is not clear. The aim of this randomized double blinded controlled clinical study was to compare the duration of postoperative analgesia with two commonly used doses of nalbuphine (0.8 and 1.6 mg) when used as an adjuvant with hyperbaric bupivacaine intrathecally. We hypothesized increasing the dosage from 0.8 to 1.6 mg may not increase the duration of analgesia due to the ceiling effect of partial opioids. The secondary objectives were to observe the hemodynamic parameters and incidence of other side effects.
METHODOLOGY:
A sample size of 60 was determined based on previous studies and alpha and beta error of 5% and 20% (power of 80) respectively and a minimum clinical difference of 30% prolongation of analgesia. Considering for dropouts, a 70 patients of ASA I and II undergoing elective lower abdominal surgeries and lower limb feasible under spinal anesthesia were recruited for the study after obtaining approval from the ethics committee and informed consent from the patients. The study was done in a sub-urban teaching hospital from the month of May to July 2015.
Inclusion criteria were American Society of Anesthesiologist grades 1 & 2, age group 18-60 years, both sexes, BMI 18.5-30, height 145 cm – 180 cm and undergoing elective lower abdominal, pelvic, perineal lower limb surgeries. Exclusion criteria were history of adverse response to nalbuphine or bupivacaine, contraindications to spinal anesthesia, pregnancy, inability to understand visual analogue score (VAS) and chronic drug therapy. Out of 70 patients, 66 fulfilled the eligibility criteria.
Visual analogue scoring was explained to the patients and informed written consent was obtained. All participants were premedicated the night before with oral diazepam and ranitidine and were fasting at least for 6 hours. Selected patients were randomized into two groups – Group A (0.8 ) and Group B (1.6) of 33 each with the help of computer generated numbers from an online random number generator.6 Opaque sealed envelopes are used. After shifting the patients inside the operating room standard monitors (ECG, pulse oximetry, non-invasive blood pressure and nasal capnography) were attached. Patients were preloaded with 500 ml of ringer lactate.
Group A (0.8) patients received 3.2 ml of hyperbaric bupivacaine 0.5% and 0.8 mg of nalbuphine intrathecally in L2-L3 space using a 25G Quincke needle in lateral position. Group B (1.6) patients received the same amount of bupivacaine with 1.6 mg nalbuphine. An insulin syringe was used for precision. The volumes in both syringes were made equal in both groups by adding normal saline. Drugs were prepared by the researcher allotting the groups and handed over to the blinded investigator, who performed the injections and collected the data.
Both the patient and the anesthesiologist administering the drug and monitoring the patient were blinded to the group allotment. Intraoperatively sensory onset (time to achieve loss of sensation to pin prick at T10 level) motor onset (time to achieve a modified Bromage score of 2, Inability to raise leg or flex knees) and maximum level of sensory loss were noted. Hemodynamic parameters (heart rate and blood pressure), oxygen saturation, respiratory rate, level of sedation and nasal Etco2 were monitored and recorded every three minutes intraoperatively. Level of sedation was noted by Campbell scoring system (1-awake, 2-Sedated but arousable, 3-Drowsy, 4-Unarousable).
If patients complained of intraoperative pain, discomfort or reached a VAS score more than 3, general anesthesia was administered and patients were allowed to drop out of the study. Bradycardia (Heart rate less than 60) and hypotension (> 30% fall in mean arterial pressure or < 55mmHg) were treated as per conventions.
Postoperatively the analgesia was assessed by VAS score and time taken for the patient to report a VAS score of 3 was taken as the endpoint. Sensory and motor levels, hemodynamic parameters, sedation levels were also observed. Incidence of nausea, vomiting, pruritus, respiratory depression and any other side effects were recorded.
Statistical analysis was performed using IBM SPSS version 20 and Microsoft Excel 2016 with statistics add-in package installed. Results were expressed as mean ± standard deviation or number (%). Parametric data were compared using Student’s unpaired t test. Anderson-Darling test and Shapiro-Wilk test were done to verify normality of data. Mann Whitney U test was used to compare non parametric data. Chi squared test was used to compare categorical data. Fisher’s exact test was done to determine statistical significance of incidence of side effects. Results were considered significant if p value was equal to or less than 0.05 and highly significant if p < 0.01. Whenever appropriate, the dosage of nalbuphine was the independent variable and the outcome measured was the dependent variable.
RESULT:
Seventy patients were enrolled and 66 fulfilled eligibility criteria. Out of the 66 patients randomized 4 patients from Group 0.8 and 2 patients from group 1.6 dropped out of study (5 patients had prolonged surgery and needed general anesthesia and one patient had a last minute cancellation). They were excluded from the study and an Intention to treat analysis was not done. Statistical analyses were done on 29 patients from 0.8 mg Group and 31 patients from 1.6 mg group.
Consort Flow Diagram
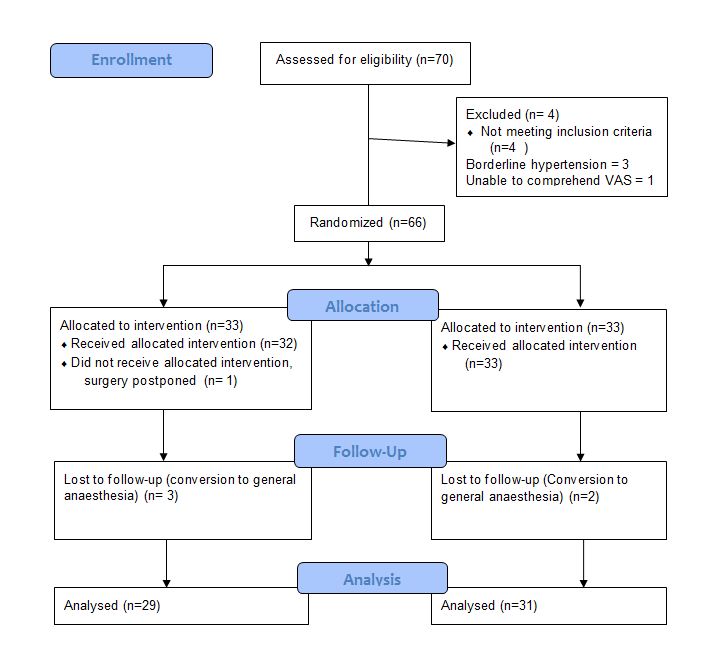
The age, sex, height and weight distributions were similar in both groups. The duration of surgery was highly variable within both groups, ranging from 30 min to 158 min. To check for normality Anderson –Darling and Shapiro Wilk tests were done and the values were found not to be normally distributed (W = 0.921, p = 0.001). Hence Mann Whitney U test was used and showed a p value of 0.246 and hence the duration of surgery did not differ between both groups (Table 1).
Table 1: Demographic data
| Parameter | Group 0.8 | Group 1.6 | p – value |
| Age (years) | 41.5 ± 10.2 | 42.9 ± 8 | 0.579 (students t) |
| Height (Cm) | 163.44 ± 7.08 | 163.87 ± 7.71 | 0.827 |
| Weight (Kg) | 59.3 ± 8.49 | 58.2 ± 6.47 | 0.57 |
| Sex (M:F) | 13:16 | 13:18 | 0.821 (Chi squared) |
| Duration of surgery
(min) |
97.03 ± 41
(Range 35-160) |
84.74 ± 37.9
(range 30-158) |
0.246 (Mann Whitney) |
The types of surgeries were inguinal hernia, abdominal and vaginal hysterectomies, varicose vein stripping etc. (Table 2).
Table 2: Various types of surgeries performed
| Procedure | Group 0.8 | Group 1.6 | Total |
| Appendectomy
Abdominal hysterectomy Vaginal hysterectomy Uterine myomectomy Hydrocele eversion Gluteal abscess I&D Multiple lipoma excision Hernioplasty Varicose vein stripping Pilonidal sinus excision Skin grafting |
3
6 3 1 2 0 1 7 3 1 2 |
3
4 3 2 5 1 0 6 2 2 3 |
6
10 6 3 7 1 1 13 5 3 5 |
| Total | 29 | 31 | 60 |
The mean sensory onset and motor onset time did not differ significantly between both the groups (Table 3). The duration of postoperative analgesia (time to reach VAS of 3) was more in the 0.8 mg group, 247.38 ± 12.2 min vs. 239 ± 10.1 min as compared to the 1.6 mg group (Figure 1).
Table 3: Sensory, motor onset and duration of analgesia
| Parameter | Group 0.8 | Group 1.6 | p value (Unpaired t) |
| Sensory onset (min) | 2.57 ± 0.23 | 2.62 ± 0.28 | 0.429 |
| Motor onset (min) | 2.79 ± 0.234 | 2.85 ± 0.24 | 0.379 |
| Duration of analgesia (min) | 247.38 ± 12.2 | 239.23 ± 10.1 | 0.007* (Significant) |
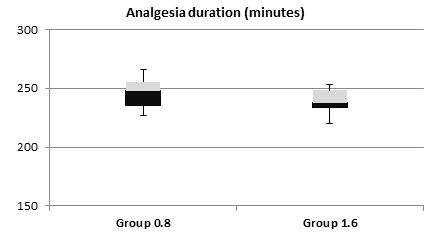
Figure 1: Postoperative analgesia duration
Regarding hemodynamic stability the baseline heart rates were statistically comparable within both groups (p = 0.74); however, intraoperatively the heart rate was persistently lower in 1.6 mg group, with highly significant differences at 30 min and 45 min (p < 0.01) and significant at 150 min, 180 min and 240 min (Figure 2). In fact 5 patients in the 1.6 mg group had symptomatic bradycardia and received injection atropine as compared to one patient in 0.8 mg group. However, the incidence of bradycardia was not statistically significant, (p = 0.196, Fisher’s exact test). Mean arterial pressures were low at 210 min interval (p < 0.01) and 180 min interval (p = 0.04). However, the clinical difference was less than 8 mmHg and none of the patients required intervention (Figure 3). The incidence of other side effects, e.g. nausea and shivering were not statistically significant between the groups (Table 4).

Figure 2: Heart rate changes
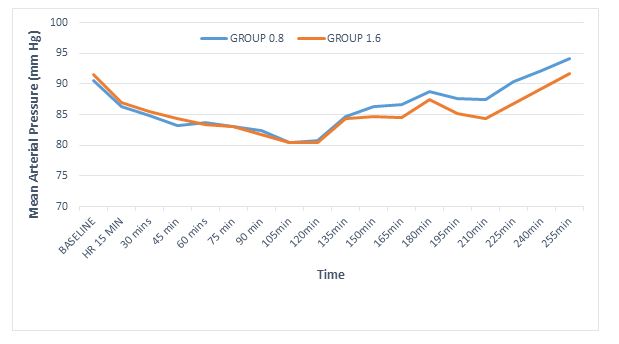
Figure 3: Mean arterial pressure changes
Table 4: Adverse events
| Adverse event | Group 0.8
(n=29) |
Group 1.6
(n=31) |
p value
(Fisher’s exact test) |
| Bradycardia | 1 | 5 | 0.196 |
| Nausea | 0 | 2 | 0.492 |
| Shivering | 0 | 3 | 0.238 |
Nasal EtCO2 was monitored in all patients and the trend was used to detect respiratory depression. The values were 29.13 ± 2.3 and 29.16 ± 2.6 in 0.8 mg and 1.6 mg groups respectively. The values in both groups did not alter significantly from the baseline. Similarly respiratory rate and oxygen saturation changes were minimal and not significant.
A post hoc power analysis was done. With Cohen’s effect size of 0.78, 2 sided t test using the mean and standard deviations of the primary outcome, a value of 0.84 was obtained which was acceptable.
DISCUSSION:
Intrathecal nalbuphine had been found to be equally effective to morphine regarding postoperative analgesia and a superior side effect profile. Various doses have been used and a progressively increasing duration of postoperative analgesia has been suggested up to doses of 0.8. mg.7 On the other hand the incidence of adverse effects increases with higher doses. Our study has compared a ‘conventional’ dose of 0.8 mg and a ‘high’ dose of 1.6 mg as an adjuvant to 0.5% hyperbaric bupivacaine with respect to postoperative analgesia.
The primary outcome, duration of postoperative analgesia was approximately 4 hours in both the groups. The results correlate with studies by Gomaa H et al.8 who reported analgesia duration of 231.83 ± 15.73 min with 0.8 mg nalbuphine and Tiwari et al.9 who reported a duration of 278.5 ± 6.04 with 0.4 mg nalbuphine.
Inability of higher doses of nalbuphine to prolong analgesia demonstrate a ceiling effect, where in higher doses cannot achieve more analgesia, but can increase the incidence of adverse effects. Interestingly nalbuphine can have an anti-analgesic effect in higher doses, which might partly explain inability of the high dose to achieve more analgesia. It has been recently suggested by Gear R et al., that “Nalbuphine-induced activation of caudate (perhaps by disinhibition, as opioids are inhibitory) initiates pain-enhancing connectivity with other regions, and, although the receptor(s) involved is not known, and blockade of this connectivity by naloxone abolishes this pronociceptive effect”.10
The anti-analgesic effect is pronounced in males. A 5 mg dose of nalbuphine caused more postoperative pain than placebo in male patients.11 This might be due to sex related due to sexual dimorphism of kappa opioid receptors12 upon which nalbuphine exerts its predominant action.
The sensory and motor onset did not differ significantly between both groups. Several studies have monitored 2 segmental regression times intraoperatively. We feel checking for segmental levels intraoperatively in abdominal surgeries and in a calm, sedated patient is cumbersome and impractical.
Heart rate was significantly lower in 1.6 mg group at several instances. Bradycardia is a known side effect of nalbuphine. 5/31 patients of 1.6 mg group had bradycardia and 1/31 had nausea compared 1/29 and nil in 0.8 mg group respectively. Even though the difference mean heart rates were significant, the incidence of bradycardia was not statistically significant. However, significance cannot be attributed to this factor as the study is not powered to detect adverse events.
Nasal EtCo2 monitoring’s accuracy depends upon the design of the cannula.13 Zhang et al. reported a significant correlation between nasal PetCO2 and PaCo2. The correlation coefficients had approximate values, 0.832 (P < 0.0001) for PaCO2 with PetCO2 through the nose and 0.836 (P < 0.0001) for PaCO2 with PetCO2 through the pharynx.14 We have monitored nasal PetCO2 to detect respiratory depression due to nalbuphine and the values were not significantly raised from baseline.
LIMITATIONS:
Conversion to general anesthesia was required in 5 patients and an intention to treat analysis was not done. Various strategies have been suggested to deal with missing data and each has its limitations. The resultant unequal sample size might make the treatment effect difficult to interpret. Visual analogue scale, the primary measurement tool is a subjective scale and can vary between patients with same degree of painful stimuli, however it is a validated tool and widely used to assess pain. Two segmental regression time was not calculated as we find it unpleasant to test sensory levels in the middle of abdominal surgeries, though several studies mention it.
CONCLUSION:
Intrathecal nalbuphine in doses of 0.8 mg and 1.6 mg as an adjuvant to 0.5% hyperbaric bupivacaine prolongs the duration of postoperative analgesia by approximately 4 hours, which can be highly valuable in preventing acute postoperative pain and its adverse effects. A dose of 0.8 mg provides better postoperative analgesia with less adverse events than a 1.6 mg dose.
Conflict of interest: Nil declared by the authors
Authors’ Contribution: PV – Concept, study designing, manuscript preparation, statistical analysis design. KB – Conduction, data collection..
REFERENCES:
- Gupta A, Kaur K, Sharma S, Goyal S, Arora S, Murthy RS. Clinical aspects of acute post-operative pain management & its assessment. J Adv Pharm Technol Res. 2010 Apr;1(2):97-108. [PubMed] [Free full text]
- Breivik H, Stubhaug A. Management of acute postoperative pain: still a long way to go! 2008 Jul 15;137(2):233-4.doi: 10.1016/j.pain.2008.04.014. [PubMed]
- Zeng Z, Lu J, Shu C, Chen Y, Guo T, Wu QP. A Comparision of Nalbuphine with Morphine for Analgesic Effects and Safety : Meta-Analysis of Randomized Controlled Trials Sci Rep. 2015; 5: 10927. doi: 10.1038/srep10927. [PubMed] [Free full text]
- Jyothi B, Gowda S, Shaikh SI, et al. A comparison of analgesic effect of different doses of intrathecal nalbuphine hydrochloride with bupivacaine and bupivacaine alone for lower abdominal and orthopedic surgeries. Indian J Pain 2014;28:18-23. [Free full text]
- Gupta K, Rastogi B, Gupta PK et al. Intrathecal nalbuphine versus intrathecal fentanyl as adjuvant to 0.5% hyperbaric bupivacaine for orthopedic surgery of lower limbs under subarachnoid block: A comparative evaluation. Indian J Pain. 2016;30(2):90-95. [Free full text]
- RESEARCH RANDOMIZER. [Online]. [cited 20th May 2015] Available from: URL: http://www.randomizer.org
- Mukherjee A, Pal A, Agrawal J, Mehrotra A, Dawar N. Intrathecal nalbuphine as an adjuvant to subarachnoid block: What is the most effective dose? Anesth Essays Res. 2011 Jul-Dec; 5(2): 171–175. doi: 10.4103/0259-1162.94759. [PubMed] [Free full text]
- Gomaa HH, Mohamed NN, Zoheir HAH, Ali MS. A comparison between post-operative analgesia after intrathecal nalbuphine with bupivacaine and intrathecal fentanyl with bupivacaine after cesarean section. Egypian J Anaesth. 2014; 30(4):405-410. [Free full text]
- Tiwari AK, Tomar GS, Agrawal J. Intrathecal bupivacaine in comparision with a combination of nalbuphine and bupivacaine for subarachnoid block: A randomized prospective double blind clinical study. Am J Ther 2013;20:592-5. doi: 10.1097/MJT.0b013e31822048db. [PubMed]
- Gear R, Becerra L, Upadhyay J, Bishop J, Wallin D, Pendse G, et al. Pain facilitation brain regions activated by nalbuphine are revealed by pharmacological fMRI. PLoS One. 2013; 8(1): e50169. doi: 10.1371/journal.pone.0050169. [PubMed] [Free full text]
- Gear RW, Gordon NC, Hossaini-Zadeh M, Lee JS, Miaskowski C, Paul SM, et al. A subanalgesic dose of morphine eliminates Nalbuphine anti-analgesia in postoperative pain. J Pain. 2008;9(4):337-41. doi: 10.1016/j.jpain.2007.11.011. [PubMed] [Free full text]
- Rasakham K, Liu-Chen LY. Sex differences in kappa opioid pharmacology. Life Sci. 2011 Jan 3; 88(0): 10.1016/j.lfs.2010.10.007. doi: 10.1016/j.lfs.2010.10.007. [PubMed] [Free full text]
- Ebert TJ, Novalija J, Uhrich TD, Barney JA. The effectiveness of oxygen delivery and reliability of carbon dioxide waveforms: a crossover comparison of 4 nasal cannulae. Anesth Analg. 2015 Feb;120(2):342-8. doi: 10.1213/ANE.0000000000000537. [PubMed]
- Zhang C, Wang M, Wang R, Wang W. Accuracy of end-tidal CO2 measurement through the nose and pharynx in nonintubated patients during digital subtraction cerebral angiography. J Neurosurg Anesthesiol. 2013 Apr;25(2):191-6. doi: 10.1097/ANA.0b013e31827c9d5a. [PubMed]
↧
Efficacy and safety of dexmedetomidine as an intrathecal agent: a dose finding clinical study
Arvinder Pal Singh, MD1, Sunil Chawla, MD2, Sukhminder Jit Singh Bajwa, MD, MBA, FACEE3, Menaal Khanna, MBBS4
1Associate Professor; 2Professor
Sri Guru Ram Das Institute of Medical Sciences & Research, Mehta Road, PO Vallah, Amritsar – 143501. Punjab, India
3Director Professor; 4Junior Resident,
Department of Anesthesiology and Intensive Care, Gian Sagar Medical College and Hospital, Banur, Patiala, Punjab, India.
Correspondence: Dr. Sukhminder Jit Singh Bajwa, House No. 27-A, Ratan Nagar, Tripuri, Patiala, Punjab, (India) PIN-147001; Ph: No-+919915025828, +911752352182; E-mail: sukhminder_bajwa2001@yahoo.com
ABSTRACT
Background and Objectives: Dexmedetomidine is increasingly being used in regional anesthesia as an adjuvant but there is no consensus on exact minimal and safe dose when used intrathecally. The present study was conducted to evaluate the efficacy of three different doses of dexmedetomidine when given intrathecally as an adjuvant to bupivacaine in patients undergoing lower abdominal surgery.
Methodology: After taking ethical committee approval, and obtaining patients consent, 60 American Society of Anesthesiologist (ASA) physical status I and II patients in the age group of 25-60 years undergoing lower abdominal surgeries were divided randomly into three groups in this randomized double blind study. An intrathecal dose of 2.5 ml of 0.5% hyperbaric bupivacaine was administered to all patients supplemented with dexmedetomidine. In Group A 5 mg, Group B 7.5 mg and in Group C 10 mg of dexmedetomidine was administered with a volume of 3ml of study drug in each group. The onset time, time to peak sensory level, motor blockade, sedation, duration of motor block, analgesia and any adverse effects were noted. At the end of the study, data were compiled and analyzed with appropriate statistical tests.
Results: Demographic profile was comparable in all the three groups. The time to onset of sensory block in Group C (1.55 ± 0.510 min) was significantly lower than Group A (2.15 ± 0.745 min) and Group B (2.20 ± 0.410 min). Sensory regression by two segments was significantly higher in Group C (220.65 ± 25.86 min) as compared to Group A (104.7 ± 25.5min) and Group B (145.10 ± 24.54 min). (p < 0.05) The duration of motor block was shortest in Group A (243.8 ± 22.0 min) as compared to Group B (305.4 ± 35.8 min) and Group C (387.0 ± 39.4 min). The visual analogue scale score for pain was lesser in Group C as compared to the other two groups.
Conclusion: Optimal dose of dexmedetomidine is difficult to define especially with prolonged duration of sensory and motor blockade in a dose dependent manner with minimal increase in side effects with higher doses. However, we conclude that 7.5 mg seems to be just optimal intrathecal dose of dexmedetomidine and can be used safely and effectively in lower abdominal surgeries.
Key words: Bupivacaine; Dexmedetomidine; Intrathecal; Postoperative analgesia.
Citation: Singh AP, Chawla S, Bajwa SJS, Khanna M. Efficacy and safety of dexmedetomidine as an intrathecal agent: a dose finding clinical study. Anaesth, Pain & Intensive Care 2017;21(1):13-18
Received: 31 Jan 2017; Reviewed: 2 Feb 2017; Corrected: 11 Feb 2017; Accepted: 14 Feb 2017
INTRODUCTION
With advancements in modern surgical and anesthetic techniques, trend is towards use of minimal and safe dose of local anesthetics (LA) made possible by addition of adjuvants to the LA solution.1 Higher dose of local anesthetics is associated with more complications and neurological sequelae.2 Addition of adjuvants to intrathecal anesthetics not only reduce the dose of local anesthetics but also minimize the incidence of complications as well as prolong post-operative analgesia.3,4 Alpha-2 agonists are widely used nowadays as they are free from the side effects associated with use of intrathecal opioids.5 Dexmedetomidine, a highly selective alpha-2 adrenoceptor agonist, is an imidazole compound. It produces dose dependent sedation; anxiolysis and analgesia without respiratory depression when used as a supplement or adjuvant.6 Alpha-2 adrenoreceptor agonists are also known to reduce anesthetic requirements because of their sympatholytic actions.7
Researchers have used dexmedetomidine intrathecally in varying doses with varying results. Though different studies have been published worldwide, there is no uniform consensus on optimal dose of intrathecal dexmedetomidine. Commonly 5 mg of intrathecal dexmedetomidine has been evaluated considering its dose equivalence to clonidine as 1:10 through intrathecal route. However, some researchers have used even 15-20 µg of intrathecal dexmedetomidine as an adjuvant which clearly establishes a non-consensus on optimal intrathecal dose of dexmedetomidine as an adjuvant.8
Keeping in consideration, the various merits of dexmedetomidine, the present study was performed to compare the analgesic efficacy of intrathecally administered dexmedetomidine as adjuvant in three different comparative doses with hyperbaric bupivacaine (0.5%) in patients undergoing lower abdominal surgeries so as to determine an optimal dose when used as an intrathecal adjuvant.
METHODOLOGY
The present study was conducted after obtaining the approval of institutional ethics committee. A written and informed consent was obtained from all patients for this prospective randomized, double blind study in which 60 ASA I and II patients in the age group of 25-60 years of either gender, undergoing elective lower abdominal surgery were included. Preoperatively patients were counseled and familiarized with the use of visual analogue scale (VAS) pain score for the assessment of perioperative pain. A sealed envelope was randomly selected and opened by an assistant, with instructions to draw up the relevant drug. The syringe was labeled with the patient’s coded number and handed to the investigator who performed the block. Three independent observers (senior anesthesiologist posted on duty, not included in the study) then observed the onset and offset of sensory and motor blockade and analgesia as per the written protocol supplied to them. Data was compiled when blinding was revealed at the end of the study. Considering a difference of 30 mins in post-op analgesia, a sample of 18 was considered adequate for the study keeping α-error at 0.05 and power of the study at 80%. However we took 20 patients in each group for better validation of results.
All the three groups received 2.5 ml of 0.5% hyperbaric bupivacaine with varying concentrations of dexmedetomidine and addition of saline to make a universal volume of 3 ml in each group. Group A patients were administered 5 mg of dexmedetomidine, Group B was administered 7.5 mg of dexmedetomidine while in Group C, patients were administered 10 mg of dexmedetomidine.
Patients on alpha adrenergic receptor blockers, local sepsis at the site of proposed puncture, known hypersensitivity to drug, treated with anticoagulants, CNS active drugs, suffering from bleeding diathesis or coagulation disorders, spinal deformity or tuberculosis of spine, having increased intracranial pressure were excluded from the study.
Preoperative assessment was done for each patient and patients were given tab. alprazolam 0.25 mg and tab ranitidine 150 mg at night before surgery and 6 am on the day of surgery. Patients were kept fasting as per the standard protocols and guidelines. Before shifting all the patients to operation theater, baseline parameters were observed and recorded which included an ECG (5 lead), noninvasive blood pressure and pulse oximeter and other vital parameters. An intravenous line was secured with 18 gauge cannula and patients were preloaded with ringer lactate 10 ml/kg 15-20 min before anesthesia. Subarachnoid block was performed with patients in sitting or left lateral position, using 25G Quincke needle and adopting a midline approach at L2-L3/L3-L4 intervertebral space. Patients were turned to supine position immediately and supplemental oxygen was administered. The following parameters were observed: time to onset of sensory blockade and motor blockade, time to maximum level of sensory blockade, time to attain complete motor blockade, two dermatomal segment regression time, total duration of motor blockade, sedation levels, post-op analgesia assessment using VAS, recue dosage of analgesia and any side effects occurring peri-operatively.
Sensory blockade was assessed using pinprick method with a blunt tipped needle every minute for the first 10 min, then at 5 min for the next 60 min and then every 15 min until regression to two segments from the maximum level achieved. Quality of motor blockade was assessed using modified Bromage scale. Inj fentanyl 100 µg was used as rescue analgesic in case of any complaint of pain.
Hemodynamic parameters were observed continuously and recorded every minute for first 10 min, then at 5 min for the next 60 min and then every 15 min till the end of surgery and then hourly during postoperative period for the next 6 hours.
Statistical analysis was done using student’s t- test for parametric data. Intergroup analysis was done using paired t-test. Chi-square test was used to analyze the categorical data and wherever frequencies were less than 5, Fisher’s exact test was used. Hemodynamic and other vitals were compared using ANOVA and applying post hoc significance. Kruskal Wallis H-test was used to assess the VAS scale. Values of p < 0.05 were considered statistically significant, and p < 0.001 was considered highly significant.
RESULTS
All the three groups were comparable in terms of age, weight, height and duration of surgery (Table 1). The distribution of the patients according to ASA grades was statistically insignificant (p > 0.05).
Table 1: Demographic variables in all the groups
| Variable | Group A
(n = 20) |
Group B
(n = 20) |
Group C
(n = 20) |
Intergroup significance |
| Age (years) | 46.35 ± 9.103 | 46.05 ± 8.249 | 45.50 ± 8.971 | NS |
| Gender (M/F) | 11/9 | 9/11 | 10/10 | NS |
| Weight (kg) | 68.70 ± 7.491 | 69.60 ± 8.444 | 68.95 ± 6.219 | NS |
| Height (cm) | 157.50 ± 2.819 | 158.55 ± 3.379 | 157.35 ± 4.017 | NS |
| Duration of surgery (min) | 79.25 ± 15.600 | 82.75 ± 10.062 | 81.00 ± 15.694 | NS |
| ASA Grade I* | 15 (75) | 14 (70) | 14 (70) | NS |
| ASA Grade II* | 5 (25) | 6 (30) | 6 (30) | NS |
Data: Mean ± SD; NS- Non-significant (p ˃ 0.05); *n (%)
The mean time of onset of sensory block in Group C was lower than Group A and Group B and the difference was statistically highly significant (p < 0.001). However, when Group A and B were compared it was statistically insignificant (p > 0.05) The mean time taken for regression of sensory block by two segments was statistically significantly higher in Group C as compared to the other two groups (p < 0.001)(Table 2).
The mean time taken for onset of motor block to grade 3 in all the three groups was statistically insignificant whereas the duration of motor block when compared in all the three groups was statistically significant (p < 0.001), Group A having the shortest duration of motor blockade. The duration of analgesia was significantly increased in Group C as compared to Group B and Group A (p < 0.001) (Table 2).
The mean pain score among all the three groups was statistically insignificant till 90 min postoperatively. At 105 min, there was increase in visual analogue scale (VAS) in Group A which was statistically significant as compared to Group B and Group C. At 240 min the difference between Group B and C became statistically significant. At 24 hours the pain score among the three groups showed statistically significant difference with lowest VAS in Group C (p < 0.05) (Table 3).
Table 2: Showing comparison of regional anesthesia characteristics in all the groups
Regional anesthesia parameters
| Group A
mean ± SD |
Group B
mean ± SD |
Group C
mean ± SD |
Intergroup Significance | |||
| A to B | A to C | B to C | ||||
| Onset of sensory blockade (mins) | 2.15 ± 0.745 | 2.20 ± 0.410 | 1.55 ± 0.510 | NS | HS | HS |
| Time to 2 segment sensory regression (mins) | 104.7 ± 25.5 | 145.10 ± 24.542 | 220.65 ± 25.869 | HS | HS | HS |
| Motor Block to reach Bromage 3 (mins) | 3.10 ± 0.852 | 3.30 ± 1.031 | 2.75 ± 1.020 | NS | NS | NS |
| Regression to bromage scale 0 (mins) | 243.8 ± 22.0 | 305.4 ± 35.8 | 387.0 ± 39.4 | HS | HS | HS |
| Duration of Analgesia (mins) | 200.0 ± 26.8 | 310.0 ± 65.8 | 412.7 ± 68.4 | S | HS | S |
Data: Mean ± SD, NS-Non-significant (p > 0.05), HS-Highly significant (p < 0.001)
Table 3: Showing visual analogue scale at various time interval post-operatively
| Time (min) | Group A
mean ± SD |
Group B
mean ± SD |
Group C
mean ± SD |
Intergroup Significance | ||
| Group A to B | Group A to C | Group B to C | ||||
| 75 | 0.30 ± 0.57 | 0 | 0 | NS | NS | NS |
| 90 | 0.80 ± 0.75 | 0 | 0 | NS | NS | NS |
| 105 | 2.9 ± 1.21 | 0 | 0 | S | S | NS |
| 120 | 3.85 ± 0.98 | 0 | 0 | S | S | NS |
| 240 | 4.80 ± 0.69 | 1.90 ± 0.68 | 0 | S | S | S |
| 360 | 5.60 ± 0.59 | 3.50 ± 0.68 | 0 | S | S | S |
| 480 | 6.80 ± 0.69 | 4.75 ± 0.71 | 2.90 ± 0.85 | S | S | S |
| 720 | 7.55 ± 0.68 | 5.85 ± 0.81 | 4.35 ± 0.74 | S | S | S |
| 1440 | 7.90 ± 0.30 | 6.85 ± 0.88 | 6.25 ± 0.81 | NS | S | S |
Data: Mean ± SD, S-significant (p < 0.05), NS-Non-significant (p ˃ 0.05)
Table 4: Showing total no. of doses of rescue analgesia and total dosage
| Group A | Group B | Group C | Intergroup Significance | |||
| n = 20 | n = 20 | n = 20 | A to B | A to C | B to C | |
| No. of doses | 12.6 ± 1.4 | 8.4 ± 1.1 | 6.75 ± 1.0 | HS | HS | S |
| Total Dosage | 900 ± 4.5 | 630 ± 8.4 | 502 ± 7.6 | HS | HS | S |
Data: Mean ± SD, HS- Highly significant (p < 0.01), S- Significant (p < 0.05)
Figure 1: Showing the incidence of adverse effects in all the three groups
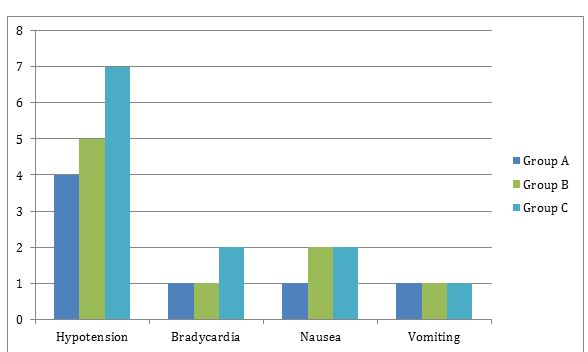
On intergroup analysis the requirement of rescue analgesia was significantly lower statistically in Group C as compared to Group B and Group A (p < 0.001) (Table 4). The intergroup comparison of adverse effects was found to be statistically insignificant (p > 0.05) and there was no incidence of adverse effects like dry mouth, urinary retention, and respiratory depression (Figure 1).
DISCUSSION:
In order to maintain the advantage of low dose local anesthetics while improving intra operative quality of anesthesia, different agents have been used as adjuvants for prolonging the duration of spinal anesthesia.9 The usage of lower doses of local anesthetic minimizes the incidence of side effects associated with higher dosages.10
Increasing use of dexmedetomidine has almost revolutionized the modern anesthesia practice. However, its off-label use as an intrathecal agent still remains questionable in terms of dosage. It has been used in varying doses with varying results with local anesthetic agents such as bupivacaine.
Dexmedetomidine and clonidine have been extensively studied and employed clinically to achieve the desired effects in regional anesthesia.11-14 The mechanism of action include their binding to presynaptic C fibers and postsynaptic dorsal horn neurons which causes decreased release of C fiber neurotransmitters and hyper polarization of postsynaptic dorsal horn neurons.15, 16 However, no study till date has compared the different lower intrathecal doses of dexmedetomidine for optimal clinical effectiveness. In the present study, the time taken from the completion of injection of study drug till the patient felt loss to pin prick sensation at T10 was considered as time of onset of sensory block. On comparing all the groups there was decrease in onset time with dose dependent increase of intrathecal doses of dexmedetomidine whereas no significant difference in the level of sensory blockade was found with increasing dose of dexmedetomidine. This finding was in concordance with Al- Mustafa et al.17 and Saadawy I et al.18 (Table 2).
There was a significant increase in regression time with 10 mg dose in comparison with 5 mg and 7.5 mg. This observation was in accordance with the study results of Al-Mustafa et al.17 and Eid MD et al.19 The possible reason for this finding could be that dexmedetomidine stimulates alpha-2 receptors directly in the spinal cord, thus inhibiting the firing of nociceptive neurons. The local anesthetics act by blocking sodium channels, whereas the alpha-2 adrenoceptor agonists act by binding to presynaptic C fibers and postsynaptic dorsal horn neurons.20 The effect of dexmedetomidine is additive or synergistic to the action of local anesthetics and increases in dose dependent manner (Table 2).
In the present study no statistical difference was observed in the duration of onset of motor block to grade 3. Similar results were seen by Eid et al.19 and Sunil et al.21 (Table 2). This is a surprising result as dose dependency is seen more in sensory effect and minimal in onset of motor blockade with intrathecal dexmedetomidine.
The patients receiving 10 mg of dexmedetomidine showed maximum prolongation in duration of motor block (387 min) followed by 7.5 mg of dexmedetomidine (305 min) and least prolongation in patients receiving 5 mg of dexmedetomidine (243 min). The most probable reason for this might be direct impairment of excitatory amino acid release from spinal interneurons. (Table 2). This observation was comparable with earlier studies done by Al-Mustafa et al.17, Eid MD et al.19 and Sunil et al.21
The total dosage of rescue analgesics was significantly decreased with higher dose of dexmedetomidine; this was in accordance to Gupta et al.4 This could have been because of the administration of alpha-2 adrenergic agonist through intrathecal and epidural route provides augmentation of analgesic effect in postoperative period. At spinal cord level, activation of both a2-C and a2-ARs, in the neurons of superficial dorsal horn especially lamina II, directly reduces pain transmission, by suppressing the release of pro-nociceptive transmitter, substance P and glutamate from primary afferent terminals and by hyperpolarizing spinal interneurons via G-protein mediated activation of potassium channels.22, 23
The incidence of adverse effects was comparable in all the three groups and was statistically non-significant. Cardiovascular depression from alpha-2 adrenergic agonists can occur at both brain and spinal cord sites. Postsynaptic activation of a2adrenoceptors in the central nervous system inhibits sympathetic activity and thus can decrease blood pressure and heart rate.24
Major limitations of our study were that we could not analyze biochemically the blood concentration of drugs due to non-availability of such advanced facilities at our institution. The optimal dose is difficult to define as postoperatively sensory and motor blockade increases in dose dependent manner. However, these effects can be utilized in different clinical situations on individual basis where early or late discharge, early or late mobility or prolonged sensory and motor blockade is warranted. Both 7.5 and 10 mg of dexmedetomidine can be used intrathecally for better surgical anesthesia and post-operative comfort. Though on statistical comparison, incidence of side effects is not significant, clinically 10 mg of dexmedetomidine is associated with a higher incidence of side effects as compared to 7.5 and 5 mg of dexmedetomidine. On the other hand, 7.5 mg of dexmedetomidine is more effective as compared to 5 mg dose which is clearly evident from the regional anesthesia characteristics in the present study.
CONCLUSION:
To conclude, addition of dexmedetomidine prolonged the sensory and motor block significantly when used with hyperbaric bupivacaine intrathecally in a dose dependent manner, without increasing the incidence of significant adverse effects. From the findings of the present study, 7.5 mg of dexmedetomidine seems to be a better intrathecal adjuvant dose to local anesthetics clinically as compared to other two doses with regards to optimal synergistic effects and minimal side effects.
Conflict of interest: Nil
Author contribution: All authors took part in design, planning, conduct of the study and data collection, literature review and manuscript preparation
REFERENCES:
- Gupta M, Shailaja S, Hedge K.S. Comparison of intrathecal Dexmedetomidine with Buprenorphine as adjuvant to Bupivacaine in Spinal Anaesthesia. J Clin Diagn Res. 2014 Feb;8(2):114-7. doi: 10.7860/JCDR/2014/7883.4023 [PubMed] [Free full text]
- Lambert, Donald H. Complications of spinal anesthesia. International. Anesthesiology. Clinics. 1989; 27(1): 51-55. [Free full text]
- Bajwa SJ, Bajwa SK, Kaur J, Singh A, Bakshi G, Singh K, et al. Admixture of clonidine and fentanyl to ropivacaine in epidural anesthesia for lower abdominal surgery. Anesth Essays Res. 2010 Jan-Jun;4(1):9-14. [PubMed] [Free full text]
- Gupta R, Verma R, Bogra J, Kohli M, Raman R, Kushwaha JK. A comparative study of intrathecal dexmedetomidine and fentanyl as adjuvants to bupivacaine. J Anaesthesiol Clin Pharmacol. 2011 Jul;27(3):339-43. doi: 10.4103/0970-9185.83678. [PubMed] [Free full text]
- Bajwa S, Arora V, Kaur J, Singh A, Parmar SS. Comparative evaluation of dexmedetomidine and fentanyl for epidural analgesia in lower limb orthopedic surgeries. Saudi J Anaesth. 2011 Oct;5(4):365-70. doi: 10.4103/1658-354X.87264. [PubMed] [Free full text]
- Bajwa S, Kulshrestha A. Dexmedetomidine: An adjuvant making large inroads into clinical practice. Ann Med Health Sci Res. 2013 Oct;3(4):475-83. [PubMed] [Free full text]
- Kamibayashi T, Maze M. Clinical uses of α2- adrenergic agonists. Anesthesiology 2000 Nov;9(5)3:1345-9 . [PubMed] [Free full text]
- Eid HA, Shafie M, Yousef H. Dose –Related prolongation of Hyperbaric Bupivacaine Spinal Anaesthesia By Dexmedetomidine.Ain Shams J Anesthesiol 2011;4:83-95.
- Buvanendran A, Krroin JS. Useful adjuvants for post-operative pain management. Best Pract Res Clin Anaesthesiol. 2007 Mar;21(1):31-49. [PubMed]
- Bernards CM. Epidural and spinal anaesthesia. In: Barash PG, Cullin BF, Stoelting RK editors. Clinical Anaesthesia. 5th Philadelphia: Lippincott Williams & Wilkins; 2009.p. 928-37.
- Bajwa SJ, Bajwa SK, Kaur J, Singh A, Bakshi G, Singh K, et al. Admixture of clonidine and fentanyl to ropivacaine in epidural anesthesia for lower abdominal surgery. Anesth Essays Res. 2010 Jam-Jun;4(1):9-14. doi: 10.4103/0259-1162.69299. [PubMed] [Free full text]
- Hall JE, Jurich TD, Barney JA, Arian SR, Ebert TJ. Sedative amnestic and analgesic properties of small dose of dexmedetomidine infusions. Anesth Analg. 2009 Mar; 90(3):699-705. [PubMed]
- Bajwa SJ, Bajwa SK, Kaur J, Singh G, Arora V, Gupta S, et al. Dexmedetomidine and clonidine in epidural anaesthesia: A comparative evaluation. Indian J Anaesth. 2011 Mar;55(2):116-21. doi: 10.4103/0019-5049.79883. [PubMed] [Free full text]
- Gabrial JS, Gordin V. Alpha-2 agonists in regional anaesthesia and Curr Opin Anaesthesiol. 2001 Dec;14(6):751-3. [PubMed]
- Bajwa SJ, Gupta S, Kaur J, Singh A, Parmar S. Reduction in the incidence of shivering with perioperative dexmedetomidine: A randomized prospective study. J Anaesthesiol Clin Pharmacol. 2012 Jan;28(1):86-91. doi: 10.4103/0970-9185.92452. [PubMed] [Free full text]
- Eisenach James C, De Kock M, Klimscha W. Alpha sub 2-adrenergic agonist for regional anesthesia. A clinical review of clonidine (1984-1995). Anesthesiology. 1996 Sep; 85(3):655-74. [PubMed] [Free full text]
- Al-Mustafa MM, Abu-Halaweh SA, Aloweidi AS, Murshidi MM, Ammari BA, Awwad ZM, et al. Effect of dexmedetomidine added to spinal bupivacaine for urological procedures. Saudi Med J. 2009 Mar;30(3):365-70. [PubMed]
- Saadawy I, Boker A, Eishahawy MA, Almaazrooa A, Melibary S, Abdellatif AA, et al. Effect of dexmedetomidine on the characteristics of bupivacaine in a caudal block in pediatrics. Acta Anaesthesiol Scand. 2009 Feb;53(2):251-6. doi: 10.1111/j.1399-6576.2008.01818 [PubMed] [Free full text]
- Shah A, Patel I, Gandhi R. Haemodynamic effect of intrathecal dexmedetomidine added to ropivacaine intraoperatively and for postoperative analgesia. Int J Bas Clin Pharmacol 2013; 2(1):26-9. [Free full text]
- Sunil BV, Sahana KS, Jajee PR. “ Dexmedetomidine as an adjuvant with hyperbaric bupivacaine for spinal anaesthesia: a double blind controlled study”. J Evolution med dent Sci 2013, 2(40), 7604-11.
- Grewal A. Dexmedetomidine: New avenues. J Anaesthesiol Clin Pharmacol. 2011 Jul; 27(3):297-302. [PubMed] [Free full text]
- Ishii H, Kohno T, Yamakura T, Ikoma M, Baba H. Action of dexmedetomidine on the substantia gelatinosa neurons of the rat spinal cord. Euro J Neurosci. 2008 Jun; 27(12):3183-90. doi: 10.1111/j.1460-9568.2008.06260 [PubMed] [Free full text]
- Eisenach JC, Shafer SL, Bucklin BA, Jackson C, Kallio A. Pharmacokinetics and pharmacodynamics of intraspinal dexmedetomidine in sheep. Anesthesiology. 1994 Jun;80(6):134-59. [PubMed]
↧
Comparison of lidocaine and a combination of lidocaine and ketorolac pretreatment on withdrawal movement induced by rocuronium injection
Muhammad Boota, FCPS1, Muhammad Hasan Wasim, FCPS2, Liaqat Ali3
1Associate Professor; 2Registrar
Department of Anesthesiology, Foundation University Medical College /
Fauji Foundation Hospital, Rawalpindi (Pakistan)
3Graded Anesthesiologist, Combined Military Hospital, Murree (Pakistan)
Correspondence: Dr. Muhammad Hasan Wasim, Operation Theatre Complex, Fauji Foundation Hospital, GT Road, Rawalpindi, (Pakistan); Phone: 0092-3111 888 345; E-mail: dochasanwasim@gmail.com
ABSTRACT:
Introduction: Rocuronium is a widely used monoquaternary aminosteroid nondepolarizing muscle relaxant of intermediate duration with a rapid onset to achieve optimal conditions for endotracheal intubations. The injection of rocuronium bromide during induction of anesthesia has often been associated with pain-induced withdrawal movement near the site of injection. It has been hypothesized that addition of ketorolac and Lidocaine in combination as pretreatment drugs among patients undergoing general anesthesia with rocuronium injection provides a better control of withdrawal movements in comparison to patients who receive only lidocaine. The objective of this study was to compare the efficacy of pretreatment of combination of ketorolac and Lidocaine and Lidocaine alone in the frequency of withdrawal movement associated with rocuronium injection in peripheral veins during intubation.
Methodology: This study was conducted on 90 patients undergoing elective surgeries under general anesthesia in operation theater complex of our hospital. Patients were randomly divided in group A and B by lottery method. Group A received 20 mg lidocaine IV prior to rocuronium. Group B received lidocaine 20 mg and ketorolac 10 mg IV. General anesthesia was administered by induction via 5 mg/kg thiopental sodium in a separate peripheral intravenous line. Withdrawal movements were observed as mild, moderate and severe, and recorded on a well-structured performa. Efficacy was defined as no withdrawal movement on injecting rocuronium.
Results: The differences in age and gender of patients were not significant in both groups and these were not associated with efficacy of treatment in the groups. However ASA status of the patients was significantly associated with efficacy of treatment groups.
In Group-A 27 (60%) and in Group-B 36 (80%) patients had no withdrawal movement while mild movement was observed in 12 (26.7%) patients in Group-A, and in 7 (15.6%) patients in Group-B. Moderate movement was seen in 6 (13.3%) patients in Group-A, and in 2 (4.4%) patients in Group-B. The number of patients who had withdrawal movement was 18 (40%) vs. 9 (20%) in Group-A and Group-B respectively (p = 0.0384).
The criterion of efficacy was fulfilled by 27 (60%) Group-A patients, compared to 36 (80%) patients in Group-B.
Conclusion: Results of this study showed that combination of intravenous lidocaine and ketorolac prior to rocuronium injection is more effective that lidocaine alone for preventing withdrawal movements for general anesthesia.
Key words: Withdrawal movement; Ketorolac; Lidocaine; Rocuronium; Intubation; General anesthesia; Efficacy
Citation: Boota M, Wasim MH, Ali L. Comparison of lidocaine and a combination of lidocaine and ketorolac pretreatment on withdrawal movement induced by rocuronium injection. Anaesth, Pain & Intensive Care 2017;21(1):31-36
Received: 25 Nov 2016; Reviewed:1, 6 Dec 2016, 24 Jan 2017; Corrected: 12 Dec 2016, 15 Jan, 3 Feb 2017; Accepted: 8 Mar 2017
INTRODUCTION:
Rocuronium is a widely used nondepolarizing muscle relaxant known for its rapid onset of action and intermediate duration of action1. Rocuronium is indicated in adult and pediatric population to facilitate tracheal intubation during routine sequence induction and to provide skeletal muscle relaxation during surgery. In adults rocuronium is also used to facilitate tracheal intubation during rapid sequence induction (RSI) and as an adjunct in the intensive care unit for short term use. ED50 for rocuronium bromide has been estimated to be 0.3 mg/kg and dose for tracheal intubation ranges from 0.6 to 1.0 mg/kg for adults and pediatric patients.
During rapid sequence induction of anesthesia pain on injection2-4 has been reported especially when the patient has not yet completely lost consciousness and particularly when propofol1, 5 is used as the induction agent. In clinical studies, pain on injection has been noted in 75-100% of the patients who underwent rapid sequence induction of anesthesia with propofol and fewer patients experienced pain who underwent rapid sequence induction of anesthesia with fentanyl2 and thiopental.
Mechanism for pain on injection and subsequent withdrawal movement has been ascribed to the release of local kinin from endohelial cells of peripheral veins. Prostaglandins seem to have enhancing effects on kinin cascade and therefore implicated for the pain experienced by the patients.
Ketorolac belongs to nonsteroidal anti-inflammatory group of analgesics (NSAID) which act via inhibition of prostaglandin synthetase and lidocaine is a local anesthetic agent, also categorized as a membrane stabilizing drug which reversibly decreases the rate of depolarization and repolarization of excitable membranes including nociceptors. Ketorolac acts to directly inhibit the local mediators which are hypothesized to be involved in the rocuronium-induced withdrawal movement while Lidocaine acts to inhibit sodium channels and prevents transmission of painful inplulses3,4.
It has been hypothesized that lidocaine and ketorolac when used alone or in combination reduced the withdrawal movement after rocuronium injection in patients undergoing anesthesia. Above stated effect has been studied at established centers of the developed world as Jeon Y et al. observed the frequency of the movements with lidocaine alone (34.3%)1, ketorolac alone (40%)1, and found that it was significantly less with the combination of the two (8.6%)1.
This study aimed to compare the response of local subjects to pretreatment with combination of ketorolac and lidocaine and lidocaine alone4,6,7 to reduce withdrawal movements associated with rocuronium injection in peripheral veins in a tertiary care hospital of Rawalpindi, Pakistan. Rocuronium has recently gained popularity for both emergency and elective procedures in this region of the world and this study aims to ascertain response of the local population to the potentially distressing effect of rocuronium Bromide injection and simple but effective methods to abolish the above mentioned responses.
METHODOLOGY:
After the approval of ethical committee of the institution, a total of 90 patients were enrolled in this study who were admitted elective patients. Patients were divided in two groups of 45 each by non-probability consecutive sampling. This study was carried out as randomized control trial at Operation Theater Complex, of our hospital, from August 2015 till February 2016. Patients included in the study were ASA I-II aged 20-60 years from either gender scheduled for elective surgery under general anesthesia. Patients with difficult venous access, concomitant co-morbid conditions like diabetes mellitus, hypertension, malignancy, pulmonary, hepatic or renal diseases were excluded. Patients with contraindications for using NSAIDS or Lidocaine (allergic reactions/hypersensitivity) and those already taking opioid analgesic, long term NSAIDS/COX-2 inhibitors or other pain killers were also not included for this study.
After approval from hospital ethical committee, 90 patients were recruited according to selection criteria. All patients were assessed a day before surgery (at least 8 hours before surgery as preoperative anesthesia fitness procedure) and written informed consent was taken. Patients were prepared by overnight fasting. Patients were randomly divided in group A and B by lottery method. Group A received 20 mg lidocaine IV prior to rocuronium. Group B received 20 mg lidocaine and 10 mg ketorolac IV. Intravascular access with two 18G cannulae was established in the pre-operative room before arriving in the operation theater. After arrival in Operation theater, monitoring including electrocardiography, pulse oximeter, noninvasive blood pressure was attached and base line heart rate and blood pressure was noted. Patients was pre-oxygenated for 3 minutes via face mask and General anesthesia was administered with either 20 mg lidocaine alone or a combination of 20 mg lidocaine and 10 mg ketorolac with a tourniquet and released after 2 minutes, followed by induction via 5 mg/kg Thiopental sodium in the separate intravenous line. After abolishment of eyelash reflex 0.6 mg/kg rocuronium was injected over 10 seconds3,5,6 for intubation in the intravenous line from which pretreatment agents were given. An observer who was blinded to the patient group assignment observed withdrawal movement which was scored as 1 (no movement of the upper extremity or a part of it, in which injection has been given), 2 (mild movement- movement of the WRIST of the upper extremity in which the injection had been given) 3 (moderate movement- elbows and shoulders of the upper extremity in which the injection had been given) and 4 (generalized body movements). After intubation anesthesia was maintained with 60% Nitrous oxide, 40% Oxygen and 0.8-1.2% Isoflurane. Injection rocuronium 1/4th of the induction dose was repeated to maintain muscle relaxation. Vitals monitoring and appropriate interventions was done accordingly at regular intervals of 3 minutes. At the end of surgery, patients were extubated and were shifted to the post-anesthesia care unit (PACU).
Data analysis: Data was collected on a structured Performa and SPSS version 10 was used to analyze data. Effect modifiers like age, gender and ASA grade was controlled by stratification. Post stratification Chi square test was applied keeping p-value less than 0.05 as significant.
RESULTS:
In Group-A 27 (60%) and in Group-B 36 (80%) patients had no movement. While mild movement was observed in 12 (26.7%) patients in Group-A and 7 (15.6%) patients in Group-B. Moderate movement was seen in 6 (13.3%) patients in Group-A and 2 (4.4%) patients in Group-B (Table-1). There were 18 (40%) patients in Group-A and 9 (20%) patients in Group-B who had withdrawal movement (Table-2). In both treatment groups the dependent variable or efficacy was defined in terms of no withdrawal movement. In Group-A efficacy was observed in 27 (60%) patients while in Group-B efficacy was seen in 36 (80%) patients (Table-3). Efficacy of treatment was also seen in relation to the age groups of patients. In age group 20-30 years there were 5 (41.7%) patients in Group-A and 9 (75%) in Group-B who were observed with no withdrawal movements. In age group 31-40 years there were 21 (65.5%) patients in Group-A and 24 (82.8%) patients in Group-B who were observed with no withdrawal movements and in patients who were > 40 years 1 (100%) patient in Group-A and 3 (75%) in Group-B were observed with no withdrawal movements. According to p-value no statistical significant association was seen for efficacy and age group of patients. Among male patients efficacy was seen in 2 (40%) patients in Group-A and 2 (100%) patients in Group-B. While among female efficacy was seen in 25 (62.5%) female in Group-A and 34 (79.1%) in Group-B. No statistically significant association was seen between gender of the patients and efficacy of treatment. It was observed that patients whose ASA grade was 1 among them efficacy of treatment was significantly associated with treatment groups, Group-A: 61.8% and Group-B: 84.4% (p = 0.039) respectively. However, in ASA grade 2 patients, the efficacy was not significantly associated with ASA grade, e.g. Group-A 54.5% and Group-B 69.2% (p = 0.459) respectively. In Group-A mean age of patients was 33.48 ± 6.75 and in Group-B mean age of patients was 34.55 ± 6.17 years. In Group-A there were 5 (11.1%) male and 40 (88.9%) female while in Group-B there were 2 (4.4%) male and 43 (95.6%) female patients. In Group-A when patients were assessed for ASA status there were 34 (75.6%) patients who were on ASA-1 and 11 (24.4%) were on ASA-2 grade. While in Group-B there were 32 (71.1%) patients whose ASA grade was 1 and 13 (28.9%) patients ASA Grade was 2.
Table 1: Response grade (severity of movement) in treatment groups [n (%)]
| Response | Group-A (n=45) |
Group-B (n=45) |
| None | 27 (60) | 36 (80) |
| Mild | 12 (26.7) | 7 (15.6) |
| Moderate | 6 (13.3) | 2 (4.4) |
| Sever | 0 (0) | 0 (0) |
Table 2: Withdrawal movement in treatment groups [n (%)]
| Withdrawal | Group-A (n = 45) |
Group-B (n = 45) |
Chi-Square Test | p-value |
| Yes | 18 (40) | 9 (20) | 4.286 | 0.0384 |
| No | 27 (60) | 36 (80) |
Table 3: Efficacy in treatment groups
| Efficacy | Group-A
(n = 45) |
Group-B
(n = 45) |
Chi-Square Test | p-value |
| Yes | 27 (60) | 36 (80) | 4.286 | 0.0384 |
| No | 18 (40) | 9 (20) |
DISCUSSION
Rocuronium bromide has been recently gaining popularity in various secondary and tertiary care hospitals across Pakistan for its favorable properties of rapid onset and relatively prolonged duration of action required for muscle relaxation during surgery. The authors studied the effects of rocuronium bromide injection on local population at a tertiary care hospital in Rawalpindi as most of the research has been carried out in the well-established centers in the West and developed countries. Rocuronium-induced injection pain or withdrawal movement (IPWM) is well known and its incidence varies between 50 and 80 %.8,9,10 Severe and burning pain occurred sometimes during rocuronium injection.9,11 In anesthetized patients, injection pain may cause withdrawal movement of the arm, which may extend to a generalized movement presumably secondary to its injection pain.9,11,12 The withdrawal movements occur more frequently in young patients. Extreme movements during induction can cause injury, and pulmonary aspiration due to gastric regurgitation has been reported in children.8 Even after loss of consciousness during the induction of anesthesia, rocuronium causes localized or generalized movements in 84% of patients9. Numerous strategies have been proposed for decreasing the pain associated with rocuronium injection. The most popular strategies involve pretreatment with drugs, such as lidocaine, although no method is completely satisfactory.
In this study it was observed that combination of lidocaine and ketorolac prior to rocuronium injection was more effective in prevention of withdrawal movements as compared to lidocaine alone. i.e. lidocaine: 40% vs. lidocaine + ketorolac: 20%. Age and gender was not significantly associated with efficacy of treatment groups. However ASA-1 status was significantly associated with efficacy of treatment groups.
Younghoon Jeon in his study compared the efficacy of lidocaine, ketorolac, and the 2 in combination as pretreatment for the prevention of rocuronium-induced withdrawal movement. As per his findings the incidence of moderate to severe withdrawal movements was 14.3% with lidocaine, 17.2% with ketorolac, and 2.9% with lidocaine/ketorolac combination, as compared to 45.7% with the placebo. There was no significant difference in withdrawal movement between the lidocaine group and the ketorolac group.1 Results of this study are consistent with the results reported by Younghoon Jeon which shows that combination of lidocaine and ketorolac is more effective in the prevention of withdrawal movement prior to rocuronium injection.
Kyo S. Kim determined the technique which prevents the withdrawal associated with rocuronium administration in adults and children. The incidence of no movement after rocuronium was 96% in L-O, 46% in L-F, 26% in C-O, and 18% in C-F in adult and 96% in S, 58% in L, and 8% in P in children. Withdrawal after rocuronium can be eliminated by the pretreatment of lidocaine during the occlusion of the IV flow in adults and addition of sodium bicarbonate in children.15
Kyo used different other drugs with combination for the prevention of withdrawal movement. But he also reported that when lidocaine used with combination it is more effective.
Taylan Akkaya and his colleagues determined the incidence and severity of pain on injection of rocuronium and its pretreatment with saline, lidocaine or ketamine were evaluated. The incidence of withdrawal movements was 32.5%, 2.5% and 15% in the saline, lidocaine and ketamine groups, respectively. The median withdrawal movement score was significantly lower only in Group Lidocaine compared to Group Saline (p-value = 0.011). There was no difference in reported pain or withdrawal movements between men and women16 . Taylan separately compared lidocaine and ketamine and reported that incidence of withdrawal movement was less with lidocaine. However, in this study combination of both these drugs lidocaine and ketorolac gives much effective cover for withdrawal movement prior to rocuronium.
Ki Tae Jung in his study compared the preventive effect of lidocaine, ketamine, and remifentanil on the withdrawal response of rocuronium. His findings showed that incidence of withdrawal response was significantly lower in lidocaine group (Group L) (20%), ketamine group (Group K) (30%), and remifentanil group (Group R) (0%), than normal saline group (Group N) (87%). Severe withdrawal response was observed in 5 of the 30 patients (17%) in Group L, and in 9 of the 30 patients (30%) in Group K. There was no severe withdrawal response in Group R. Mean blood pressure and heart rate were significantly decreased in Group R compared to other groups.17
Huang et al. demonstrated that pretreatment with 10 mg ketorolac with venous occlusion for 2 min reduced the propofol injection pain. They compared the retention time under venous occlusion and commented that sufficiently long venous occlusion (120 s, but not 30 or 60 s) played a significant role in reducing this pain.18
Indeed, experimental data suggest that ketorolac produces analgesia, mainly peripherally, by reducing sensitizing prostaglandins, although some NSAIDs also have a central action.19-21 Ketorolac improved the tourniquet tolerance and quality of postoperative analgesia when it was combined with lidocaine as intravenous regional anesthesia.22,23 Studies indicate that 20 mg of ketorolac is effective in intravenous regional anesthesia without adverse effects, implying that a larger dose may increase the risk of local complications.24
One short coming relevant to the use of rocuronium bromide pertains to unavailability of sugammadex in local market, a cyclodextrin which has been established as the reversal of steroid-based neuromuscular blockers including vecuronium and rocuronium25, limiting the use of rocuronium as an alternative of succinylcholine in anticipated difficult airway situations warranting rapid sequence intubations. Succinylcholine is still the drug of choice for difficult airway management involving emergency and non-emergency surgeries in our institution because of reversal of its effects with in span of a few minutes despite an array of adverse effects such as such as hyperkalemia, myalgia, and rhabdomyolysis. Rocuronium bromide provides the anesthesiologists of our resource-constrained country an opportunity to avoid the oft-feared complications of succinylcholine injection, provided sugammadex becomes widely available across the secondary and tertiary care setups.
Besides lidocaine, several other drugs such as ondansetron, magnesium sulfate, sodium bicarbonate, fentanyl, and remifentanil are effective in reducing pain on rocuronium injection, but pretreatment of lidocaine or other drugs before rocuronium prolongs the time between anesthesia induction and neuromuscular block administration. In addition, most of these drugs can, even in rare cases, induce adverse effects such as allergic reaction, bradycardia, and hypotension.
Since this study was carried out on patients in whom RSI was not indicated and elective procedures were to be performed in non-emergent, non-stressful controlled environment, more studies and case reports are expected in the future to establish protocols for this promising drug in RSI situations. Rocuronium bromide heralds a new era, perhaps marking an end to the reign of succinylcholine in in-hospital and field settings for airway management.
CONCLUSION:
Results of this study showed that combination of Intravenous lidocaine and ketorolac prior to rocuronium injection is more effective than lidocaine alone for preventing withdrawal movements. Based on these results it is now clear that combination of both these drugs can effectively eliminate withdrawal movement. It is recommended that combination of these drugs should be used as pretreatment for rocuronium administration.
Declaration of interest: None declared.
Funding: This study was funded by personal and departmental sources.
Authors contribution: MB: Concept, supervision of practical conduct and primary author; MHW: principal investigator, literature search, statistical analysis, manuscript editing and corresponding author
REFERENCES:
- Jeon Y, Ha JH, Lee J-E, Lee H-C, Ryu T, Kwak K-H. Rocuronium-induced withdrawal movement: influence of ketorolac or a combination of lidocaine and ketorolac pretreatment. Korean journal of anesthesiology. 2013;64(1):25-8.
- Abu-Halaweh S, Aloweidi A, Qudaisat I, Al-Hussami M, Atyat B, Al-Mustafa M, et al. Comparison of three methods of preventing rocuronium induced pain on injection using venous occlusion technique: a randomized prospective double blind controlled study. Middle East journal of anesthesiology. 2013;22(1):87-92.
- Lee YC, Jang YH, Kim JM, Lee SG. Rapid injection of rocuronium reduces withdrawal movement on injection. Journal of clinical anesthesia. 2009;21(6):427-30.
- Zhang Y, Xiang Y, Liu J. Prevention of pain on injection of rocuronium: a comparison of lidocaine with different doses of parecoxib. Journal of clinical anesthesia. 2012;24(6):456-9.
- Choi YJ, Park HS, Lee H, Yoon SZ. Single pretreatment of remifentanil may reduce pain after propofol and rocuronium injection in rapid sequence induction. Korean journal of anesthesiology. 2012;63(5):413-8.
- So SY, Kim Y-H, Ko Y-K, Park SI, Pak HJ, Jung WS. Effect of lidocaine (40 mg) mixed to prevent injection pain of propofol on the intubating conditions and onset time of rocuronium. Korean journal of anesthesiology. 2013;64(1):29-33.
- Vivancos GG KJ, Garcia LV. Effects of 2 mg.kg⁻¹ of intravenous lidocaine on the latency of two different doses of rocuronium and on the hemodynamic response to orotracheal intubation. Rev Bras Anestesiol. 2011;61:1-12.
- Shevchenko Y, Jocson JC, McRae VA, Stayer SA, Schwartz RE, Rehman M, et al. The use of lidocaine for preventing the withdrawal associated with the injection of rocuronium in children and adolescents. Anesthesia & Analgesia. 1999;88(4):746-8.
- Steegers M, Robertson E. Pain on injection of rocuronium bromide. Anesthesia & Analgesia. 1996;83(1):203.
- Borgeat A, Kwiatkowski D. Spontaneous movements associated with rocuronium: is pain on injection the cause? Br J Anesth 1997;79(3):382-3.
- Moorthy S, Dierdorf SF. Pain on injection of rocuronium bromide. Anesthesia & Analgesia. 1995;80(5):1067.
- Kim J, Kim Y, Kwak H. Pretreatment with remifentanil to prevent withdrawal after rocuronium in children. British journal of anaesthesia. 2007;98(1):120-3.
- Lui J-T, Huang S-J, Yang C-Y, Hsu J-C, Liu P. Rocuronium-induced generalized spontaneous movements cause pul71. Steegers M, Robertson E. Pain on injection of rocuronium bromide. Anesthesia & Analgesia. 1996;83(1):203.
- Cheong K, Wong W. Pain on injection of rocuronium: influence of two doses of lidocaine pretreatment. British journal of anaesthesia. 2000;84(1):106-7.
- Kim KS, Kim YS, Jeon WJ, Yeom JH. Prevention of withdrawal associated with the injection of rocuronium in adults and children. Journal of clinical anesthesia. 2006;18(5):334-8.
- Akkaya T, Toygar P, Bedirli N, YAZICIOĞLU D, GÜMÜŞ H. Effects of pretreatment with lidocaine or ketamine on injection pain and withdrawal movements of rocuronium. Turkish Journal of Medical Sciences. 2008;38(6):577-82
- Jung KT, Kim HJ, Bae HS, Lee HY, Kim SH, So KY, et al. Effects of lidocaine, ketamine, and remifentanil on withdrawal response of rocuronium. Korean journal of anesthesiology. 2014;67(3):175-80.
- Huang Y, Buerkle H, Lee T, Lu C, Lin C, Lin S, et al. Effect of pretreatment with ketorolac on propofol injection pain. Acta anaesthesiologica scandinavica. 2002;46(8):1021-4.
- Cashman JN. The mechanisms of action of NSAIDs in analgesia. Drugs. 1996;52(5):13-23.
- Rice AS, Lloyd J, Bullingham RE, O’Sullivan G. Ketorolac penetration into the cerebrospinal fluid of humans. Journal of clinical anesthesia. 1993;5(6):459-62.
- Burian M, Geisslinger G. COX-dependent mechanisms involved in the antinociceptive action of NSAIDs at central and peripheral sites. Pharmacology & therapeutics. 2005;107(2):139-54.
- Reuben SS, Steinberg RB, Kreitzer JM, Duprat KM. Intravenous regional anesthesia using lidocaine and ketorolac. Anesthesia & Analgesia. 1995;81(1):110-3.
- Steinberg RB, Reuben SS, Gardner G. The dose-response relationship of ketorolac as a component of intravenous regional anesthesia with lidocaine. Anesthesia & Analgesia. 1998;86(4):791-3.
- Souter AJ, Fredman B, White PF. Controversies in the perioperative use of nonsterodial antiinflammatory drugs. Anesthesia & Analgesia. 1994;79(6):1178-90.
- Schaller SF, Fink H. Sugammadex as a reversal agent for neuromuscular block: an evidence-based review. Core Evid. 2013;8:57–67
↧
A comparative study to assess preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section
Teena Bansal, DA, DNB1, Akanksha Joon, MD2
1Assistant Professor; 2Ex Senior Resident
Department of Anesthesiology & Critical Care, Pt. B.D. Sharma University of Health Sciences, Rohtak-124001, Haryana, (India)
Correspondence: Dr. Teena Bansal, 2/8 FM, Medical Campus, PGIMS, Rohtak-124001, Haryana, (India); Mobile: +91-9315839374; E-mail: aggarwalteenu@rediffmail.com
ABSTRACT:
Background: A common response to stress is anxiety which is present in patients undergoing surgery. As compared to general surgical population, a higher level of preoperative anxiety has been reported in obstetric patients. The present study was conducted to assess and compare preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section.
Methodology: A total of 200 obstetric patients, having physical status II according to the American Society of Anesthesiologists, undergoing elective (n=100) or emergency [Grade 2] (n=100) cesarean section were included in the study. State version of state trait anxiety inventory scale (S-STAI) and Visual analogue scale for anxiety (VAS-A) were used as study tools.
Results: A high level of anxiety in patients undergoing emergency cesarean section as compared to elective patients [S- STAI (67.29 ± 8.51 vs 48.35 ± 10.29) and VAS –A (73.61 ± 5.31 vs 52.43 ± 4.16)] was observed in present study, the difference found to be statistically highly significant (p < 0.001). Overall 110 (55%) patients had anxiety. Out of these 40 patients (40%) belonged to elective group and 70 patients (70%) were of emergency group. Anxious patients had higher education level. The difference in hemodynamic parameters was highly statistically significant between the two groups.
Conclusion: Every patient requiring surgery whether elective or emergency should be assessed for the presence of anxiety in their routine preoperative anesthesia assessment and the patients found to have a high level of anxiety should be scheduled for an additional counselling session .
Key words: Preoperative anxiety, obstetric patient, cesarean section
Citation: Bansal T, Joon A. A comparative study to assess preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section. Anaesth, Pain & Intensive Care 2017;21(1):25-30
Received: 21 Dec 2016; Reviewed: Feb 2017; Corrected & Accepted: Feb 2017
INTRODUCTION:
Anxiety is an emotional state characterized by apprehension and fear resulting from anticipation of a threatening event. In adult patients the incidence of preoperative anxiety ranges from 11% to 80% and there is variation among different surgical groups. Higher doses of induction agents and postoperative analgesia are required in anxious patients. In patients scheduled for any type of surgery, the assessment of anxiety is important as anxious patients respond differently to anesthesia than non-anxious patients. 1
Various factors influencing anxiety in a patient planned for surgery include cultural diversity, the extent & type of surgery, age, gender, previous surgical experiences, optimism, susceptibility to and ability to cope with stress and preoperative information.2
As compared to general surgical population a higher level of preoperative anxiety has been reported in obstetric patients.3,4 One of the most common surgical procedures performed on obstetric patients is cesarean section which can be either elective or emergency. For measuring anxiety, there are several instruments. Objective methods include indirect measurement of sympatheticoadrenal activity with the help of heart rate and blood pressure while more direct measurements of this activity are plasma cortisol and urinary catecholamines.5,6,7 State trait anxiety inventory (STAI), hospital anxiety and depression scale (HADS), visual analogue scale for anxiety (VAS-A) and others can be used as subjective tools for assessment of anxiety.
Various studies have been conducted to measure the preoperative anxiety in different surgical groups using different scales.8-12
However, to the best of our knowledge, there is no study in literature to assess and compare preoperative anxiety in obstetric patients undergoing elective or emergency cesarean section. Hence, the present study was carried out.
METHODOLOGY:
This cross sectional study was conducted in the Department of Anesthesiology & Critical Care, University of Health Sciences Rohtak (INDIA) from April 2015 to March 2016. After written consent of the patient, a total of 200 obstetric patients, having ASA physical status II undergoing elective or emergency (Grade 2) cesarean section, were included in the study.
Exclusion criteria were known psychiatric illness, language barrier, patient taking any antianxiety or antidepressant medication, bad obstetric history, complicated pregnancy or having congenital fetal anomaly. Patient with medical disease like hypertension, diabetes mellitus, malignancy and chronic disease, and those unwilling to participate in the study were also excluded.
For the study a proforma consisting of 3 parts was prepared. Part 1 included demographic profile i.e. name, age, medical record number, education level, occupation, parity, information of previous surgeries if any and preoperative information. Part 2 included S-STAI scale and Part 3 included VAS-A. Patients scheduled for elective cesarean section had preanesthetic checkup by anesthetist in preanesthetic checkup (PAC) clinic. In addition, on the evening prior to surgery they were visited by anesthetist. Patients were asked to fill the form of STAI in a standardized time of 10 minutes. Patients scheduled for emergency cesarean section (Grade 2) were visited by anesthetist before surgery. The preanesthetic check-up of patients was done and they were asked to fill the form in 10 min. In addition, all the patients were shown a 100 mm straight line. They were asked to mark the line below with a vertical stroke to show how anxious they felt at the moment. STAI score of 44 and above and VAS score of 50 and above was taken as presence of anxiety.
Pulse rate and blood pressure were recorded. The patients were divided into two groups. Group I (n=100) & Group II (n=100) undergoing elective or emergency (Grade 2) cesarean section respectively.
The study tools used were S-STAI and VAS-A
Hindi version of STAI was used. For measuring anxiety, the STAI form Y is the definitive instrument. It is ideal for evaluating individuals with lower educational backgrounds due to its simplicity. It includes two forms Y-1 and Y-2 each having 20 items with four possible responses to each. Form Y-1 measures the state anxiety (how the respondent feels ‘right now’ at this moment.) Form Y-2 measures the trait anxiety (how the respondent feels ‘generally’). A weighted score of 1 to 4 is given to each STAI item. Scores can vary from a minimum of 20 to a maximum of 80 for both the S-anxiety and the T-anxiety scales. The individual’s score is sum of the scores on all items. Alpha coefficient reliability for state anxiety and trait anxiety is very high such as .92. But test retest reliability is high only for trait anxiety because a valid measure of state anxiety should reflect the influence of unique situational factors that exist at the time of testing.13
For evaluation of preoperative anxiety VAS-A is a useful and easily applicable method which allows assessment of high anxiety levels in various surgical groups. The VAS comprises a 100 mm line, at the left hand of which is a statement indicating zero anxiety (‘no anxiety at all’) and at the right hand the statement ‘most anxious I can imagine’. Patients are asked to mark the line to indicate the degree of their anxiety.8
At the end of the study, the data were calculated regarding age, level of education, previous exposure of surgery, S-STAI, VAS-A and hemodynamic parameters (systolic & diastolic blood pressure and pulse rate) and analyzed statistically. Quantitative variables were calculated as mean ± SD. Qualitative variables was presented as percentage. Quantitative variables between the two groups were compared with the help of unpaired student’s t test using software SPSS version 16.5. A p-value of < 0.05 was considered significant and p-value of < 0.001 was considered highly significant.
RESULTS:
The average age of patients in Group I was 25.18 ± 3.24 years, while in Group II, it was 23.29 ± 2.67 years, the difference being statistically insignificant. Overall 110 (55%) patients had anxiety. Out of these 40 patients (40%) were of elective group and 70 patients (70%) of emergency group [Table 1]
Anxious patients had education level matric and above. Overall 50 matriculate patients (56.18%) had anxiety. Out of these 20 (39.21%) patients belonged to Group I and 30 patients (78.94%) were of Group II. Further, more of the patients had anxiety as the level of education increased. Total 38 patients (90.47%) having intermediate qualification had anxiety. In elective group, anxiety was observed in 16 patients (88.88%) and in emergency group, anxiety was observed in 22 patients (91.66%) having intermediate qualification. 10 patients (76.92%) having anxiety were of postgraduate level, out of which 4 patients (80%) belonged to Group I and 6 patients (75%) were of Group II [Table 1]. Highest level of anxiety was observed in patients having postgraduate qualification.
98 patients (61.25%) had anxiety among the patients who had no experience of prior surgery, , out of which 36 patients (46.15%) belonged to Group I and 62 patients (75.6%) were of Group II. Further, 12 patients (30%) had preoperative anxiety among the patients who had experienced past surgery, out of which 4 patients (18.18%) belonged to elective group and 8 patients (44.44%) belonged to emergency group (Table 1).
Table 1: Demographic profile of patients in two groups
| Variable | Group I
(n=100) |
Group II
(n=100) |
||
| Total no of patients | No of patients with anxiety | Total no of patients | No of patients with anxiety | |
| Level of education
Illeterate Matriculate Intermediate Postgraduate |
26 51 18 5 |
0 20 (39.21%) 16 (88.88%) 4 (80%) |
30 38 24 8 |
12 (40%) 30 (78.94%) 22 (91.66%) 6 (75%) |
| Previous exposure of surgery
No surgery Previous surgery |
78 22 |
36 (46.15%) 4 (18.18%) |
82 18 |
62 (75.6%) 8 (44.44%) |
In the elective group (n=100), who visited PAC clinic, 40 patients (40%) had anxiety while 60 patients (60%) did not have anxiety indicating the importance of PAC visit in alleviating anxiety.
A high level of anxiety in patients undergoing emergency cesarean section as compared to elective patients [S-STAI (67.29 ± 8.51 vs 48.35 ± 10.29) and VAS-A (73.61 ± 5.31 vs 52.43 ± 4.16)] was observed in present study, the difference found to be statistically highly significant (p < 0.001) (Table 2).
Table 2: Showing VAS-A and S-STAI in patients of Group I & Group II
| Scale | Group I (n=100)
Mean ± S D |
Group II (n=100)
Mean ± S D |
p value |
| VAS-A | 52.43 ± 4.16 | 73.61 ± 5.31 | < 0.001 |
| S-STAI | 48.35 ± 10.29 | 67.29 ± 8.51 | < 0.001 |
Hemodynamic parameters i.e. systolic & diastolic blood pressure and pulse were compared in both the groups. In Group I, mean systolic blood was 104.65 ± 9.75 mm Hg compared to 119.81 ± 10.15 mm Hg in Group II. Statistically highly significant difference was observed (p < 0.001). Mean diastolic blood pressures in Group I and Group II were 73.53 ± 6.62 mmHg and 92.69 ± 6.03 mm Hg respectively, the difference was statistically highly significant (p < 0.001). The mean pulse rate was 70.24 ± 11.20/min in elective group and 85.89 ± 8.52/ min in emergency group (p < 0.001) (Table 3).
Table 3: Showing blood pressure & pulse in patients of Group I & Group II
| Variables | Group I
Mean ± S D |
Group II
Mean ± S D |
p value |
| Systolic BP (mmHg) | 104.65 ± 9.75 | 119.81 ± 10.15 | < 0.001 |
| Diastolic BP (mmHg) | 73.53 ± 6.62 | 92.69 ± 6.03 | |
| Pulse/min | 70.24 ± 11.20 | 85.89 ± 8.52 |
DISCUSSION:
A common response to stress is anxiety which is present in patients undergoing surgery. Various problems like difficult venous access, delayed jaw relaxation, coughing, autonomic fluctuations and increased anesthetic requirement during induction of anesthesia are found to be associated with preoperative anxiety. In addition, preoperative anxiety is also associated with increased pain, nausea and vomiting in the postoperative period, prolonged recovery and increased risk for infection.14
Assessment of presence of anxiety and its quantification is difficult similar to pain. A variety of subjective methods are available for measuring preoperative anxiety like HAD, STAI, VAS-A, the Amsterdam preoperative anxiety and information scale (APAIS), multiple affect adjective check list (MAACL) and linear analogue scale (LAAS)15,13,8,16,9
Various factors such as age, gender, type of surgery, optimism and preoperative information influence anxiety. Decreased level of preoperative anxiety has been observed with increase in age.3 However, in another study Domar et al. did not observe age as a determinant of preoperative anxiety.17 Female sex is an important factor related to high anxiety, as some previous studies have reported a high level of anxiety in the female gender.10,17 Boker et al. and Moerman et al. did not find type of surgery as a determinant of preoperative anxiety while in another study conducted by Kindler et al., the authors observed higher level of anxiety in patients of otolaryngological and thoracic surgeries.2,16,10 In present study the average age of patients in Group I was 25.18 ± 3.24 years while in Group II, it was 23.29 ± 2.67 years, the difference being statistically insignificant. However, in present study valid statistical analysis of association between anxiety and age, gender and type of surgery was not possible because all the patients were of same age group. In addition, all patients were females.
In the present study, overall 110 patients (55%) had preoperative anxiety with S-STAI score ≥44 . The results of present study are similar to a study conducted by Jafar et al. who observed that with S-STAI scores of 44 and above, 186 (62%) patients had preoperative anxiety.3 Preoperative anxiety was prevalent in patients with education level matriculate and above in the present study(Table 1). It may be due to the reason that regarding the complications related to surgery and anesthesia, educated patients were more aware and worried. In addition, information seeking behavior is more frequent in these patients which itself is associated with high level of anxiety.16 Our observation of preoperative anxiety in educated patients is supported by a study conducted by Domar et al.17
Low anxiety levels were found in patients having exposure to prior surgery. The patients who had no experience of previous surgery, 98 patients (61.25%) had anxiety compared to 12 patients (30%) with exposure to prior surgery (Table 1). The patients with previous surgery had less fear of unknown or misconceptions about anesthesia and surgery and so less anxious. The findings of present study are in agreement with other studies.10,16
Our findings are in agreement with the study conducted by Solgajova et al. who observed type of surgery (acute or planned) as the second most predictor of preoperative anxiety.18 A high level of anxiety in patients undergoing emergency cesarean section as compared to elective patients [S-STAI (67.29 ± 8.51 vs 48.35 ± 10.29) and VAS-A (73.61 ± 5.31 vs 52.43 ± 4.16)] was observed in present study [Table 2]. Type of surgery (i.e. planned or acute) is a significant predictor of anxiety. Patients who require acute surgery, have a short time to adapt to the situation and anxiety is highly common in them.19
It has been observed by some authors that anesthesia particularly fear of anesthesia leads to the onset of preoperative anxiety.19,20 After preanesthetic checkup, patients of planned surgery are informed about surgery and the type of anesthesia for their surgery. In addition, in the preoperative period, information about surgery leads to decreased anxiety. In patients scheduled for elective surgery in the present study they underwent preanesthetic checkup by the anesthetist in the PAC clinic. In addition, they were visited in the evening prior to surgery by the anesthetist which allayed anxiety. This finding is similar to a study conducted by Egbert et al. who observed that preoperative visit by the anesthetist plays a major role to relieve anxiety.21 On the other hand, in the present study, there was comparatively less time for the anesthetist to interact with the patient of emergency cesarean section which may be the reason of high anxiety in these patients compared to elective patients.
In the preoperative period, information about surgery leads to decreased anxiety. . To transmit the necessary information and clarify the patients’ enquiries, preanesthetic consultation clinic could be the right place. Various studies have demonstrated that consultation at the preanesthetic checkup clinic has a statistically significant positive effect on alleviating patients’ anxiety.14,22,23 But this may not be feasible for emergency patients.
To the best of our knowledge, there is no study in literature evaluating anxiety in patients undergoing emergency cesarean section in addition to evaluating methods to relieve anxiety in such patients. We evaluated preoperative anxiety in obstetric patients undergoing emergency cesarean section which adds to the strength of the present study. However, we did not evaluate methods to relieve anxiety in such patients which we consider the limitation of the study. Synder-Ramoset et al. suggested that in patients undergoing surgery, use of a documentary video can supplement a patient interview during the preanesthetic visit which may be an effective technique for conveying information.24 We can apply this method to alleviate anxiety of emergency patients in addition to providing information about surgery and anesthesia.
Preoperative pharmacological medications are given to patients to relieve anxiety. Because of depressive effects of sedatives on newborns, pharmacological medications are omitted in obstetric patients. Senel et al. conducted a study including 50 obstetric patients undergoing elective cesarean section. Group I received intravenous premedication with 0.025mg/kg midazolam while the control group (Group II) received equal amount of saline 30 minutes before surgery. The authors evaluated patient anxiety with APAIS and measured newborn well-being using Apgar and the neonatal neurologic and adaptive capacity score (NACS) and concluded that patients receiving midazolam as premedication had significantly low anxiety scores without any adverse effects on the newborns.25 Agarwal et al. evaluated the efficacy of acupressure to alleviate preoperative anxiety. The authors state that it takes around 20-30 minutes for a patient to be moved from the preoperative area to being anesthetized. If the anxiolytic effect of acupressure lasts for 30 minutes or more, then there would be a calm and less anxious patient until the time of induction of anesthesia. This would avoid the need for sedative premedication with its associated side effects.26 However, further long term trials enrolling more number of patients are warranted in this direction to evaluate measures to relieve anxiety in patients undergoing emergency cesarean section.
We should be able to identify increased anxiety in preoperative period and if effective intervention strategies are implemented to reduce it, we would prevent postoperative complications (prolonged hospitalization, more intense and longer pain perception). So every patient requiring surgery whether elective or emergency should be assessed for the presence of anxiety in their routine preoperative anesthesia assessment and the patient found to have a high level of anxiety should be scheduled for an additional counselling session from the anesthetist.
Conflict of interest: None
Authors’ declaration: The manuscript has been read and approved by all the authors, the requirement of authorship has been met and each author believes that the manuscript represents honest work.
REFERENCES:
- Maranets I, Kain ZN. Preoperative anxiety and intraoperative anesthetic requirements. Anesth Analg. 1999 Dec;89(6):1346-51. [PubMed]
- Boker A, Brownell L, Donen N. The Amsterdam preoperative anxiety and information scale provides a simple and reliable measure of preoperative anxiety. Can J Anaesth. 2002 Oct;49(2): 792-8. [PubMed]
- Jafar MF, Khan FA. Frequency of preoperative anxiety in Pakistani surgical patients. J Pak Med Assoc. 2009 Jun;59(6):359-63. [PubMed] [Free full text]
- Beilin Y, Rosenblatt MA, Bodian CA, Lagmay-Aroesty MM, Bernstein HH. Information and concerns about obstetric anesthesia: a survey of 320 obstetric patients. Int J Obstet Anesth. 1996 Jul;5(3):145-51. [PubMed]
- Nisbet HI, Norris W. Objective measurement of sedation .II. a simple scoring system. Br J Anaesth. 1963;35:618-23. [PubMed]
- Williams JG, Jones JR, Williams B. The chemical control of preoperative anxiety. Psychophysiology. 1975 Jan;12(1): 46-9. [PubMed]
- Martinez LR, Von Euler C, Norlander OP. The sedative effect of premedication as measured by catecholamine excretion. Br J Anaesth. 1966 Oct;38(10):780-6. [PubMed]
- Millar K, Jelicic M, Bonke B, Asbury AJ. Assessment of preoperative anxiety: comparison of measures in patients awaiting surgery for breast cancer. Br J Anaesth. 1995 Feb;74(2):180-3. [PubMed]
- Hicks JA, Jenkins JG. The measurement of preoperative anxiety. J R Soc Med. 1988 Sep;81(9): 517-9. [PubMed] [Free full text]
- Kindler CH, Harms C, Amsler F, Ihde-Scholl T, Scheidegger D. The visual analog scale allows effective measurement of preoperative anxiety and detection of patients’ anesthetic concerns. Anesth Analg. 2000 Mar;90(3):706-12. [PubMed]
- Hernandez-Palazon J, Fuentes-Garcia D, Falcon-Arana L, Rodriguez-Ribo A, Garcia- Palenciano C, Roca-Calvo MJ. Visual analogue scale for anxiety and Amsterdam preoperative anxiety scale provide a simple and reliable measurement of preoperative anxiety in patients undergoing cardiac surgery. Int Cardiovasc Res J 2015; 9: 1-6. [PubMed] [Free full text]
- Maheshwari D, Ismail S. Preoperative anxiety in patients selecting either general or regional anesthesia for elective cesarean section. J Anaesthesiol Clin Pharmacol. 2015 Apr-Jun;31(2): 196-200. doi: 10.4103/0970-9185.155148. [PubMed] [Free full text]
- Spielberger CD, Gorsuch RL, Lushene RE, Vagg PR, Jacobs GA. Manual for the state-trait anxiety inventory. Consulting psychologists Press, Palo Alto CA. 1983.
- Nigussie S, Belachew T, Wolancho W. Predictors of preoperative anxiety among surgical patients in Jimma University Specialised Teaching Hospital, South Western Ethiopia. BMC Surgery. 2014; 14:67. [PubMed] [Free full text]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983 Jun;67(6): 361-70. [PubMed]
- Moerman N, van Dam FS, Muller MJ, Oosting H. The Amsterdam preoperative anxiety and information scale (APAIS). Anesth Analg. 1996 Mar;82(3):445-51. [PubMed]
- Domar AD, Everett LL, Keller MG. Preoperative anxiety: is it a predictable entity? Anesth Analg. 1989 Dec;69(6):763-7. [PubMed]
- Solgajova A, Sollar T, Zrubcova D, Vorosova G. Predictors of preoperational anxiety in surgical patients. Kontakt 2015; 17: e201-e205.
- Karanci AN, Dirik G. Predictors of pre- and postoperative anxiety in emergency surgery patients. J Psychosom Res. 2003 Oct;55(4): 363-9. [PubMed]
- Caumo W, Schmidt AP, Schneider CN, Bergmann J, Iwamoto CW, Adamatti LC, et al. Risk factors for postoperative anxiety in adults. Anaesthesia. 2001 Aug;56(8):720-8. [PubMed] [Free full text]
- Egbert LD, Battit G, Turndorf H, Beecher HK. The value of the preoperative visit by an anesthetist. A study of doctor patient rapport. JAMA. 1963 Aug 17;185(7): 553-5. [PubMed]
- Kiyohara LY, Kayano LK, Oliveira LM, Yamamoto MU, Inagaki MM, Ogawa NY, et al. Surgery information reduces anxiety in the pre-operatve period. Rev Hosp Clin Fac Med Sao Paulo. 2004 Apr;59(2):51-6. [PubMed] [Free full text]
- Davidson S, Mckendrick D, French T. Preassessment clinic interview and patient anxiety. Saudi J Anaesth. 2016 Oct-Dec;10(4):402-8. [PubMed] [Free full text]
- Synder-Ramos SA, Seintsch H, Bottiger BW, Motsch J, Martin E, Bauer M. Patient satisfaction and information gain after the preanaesthetic visit: a comparison of face-to-face interview, brochure, and video. Anesth Analg. 2005 Jun;100(6):1753-8. [PubMed]
- Senel AC, Mergan F. Premedication with midazolam prior to caesarean section has no neonatal adverse effects. Braz J Anestesiol. 2014 Jan-Feb;64(1):16-21. doi: 10.1016/j.bjane.2012.08.005 [PubMed] [Free full text]
- Agarwal A, Ranjan R, Dhiraaj S, Lakra A, Kumar M, Singh U. Acupressure for prevention of pre-operative anxiety: a prospective, randomised, placebo controlled study. Anaesthesia. 2005 Oct; 60(10): 978-81. [PubMed] [Free full text]
↧
↧
Prophylactic use of gabapentin to reduce postoperative nausea and vomiting in patients undergoing diagnostic gynecological laparoscopy
Muhammad Amjad Khan1, Khalid Javid Siddiqi2, Muhammad Sabir Khan3
1Associate Professor; 2Professor; 3Senior Registrar
Department of Anesthesiology & Intensive Care, FMH College of Medicine & Dentistry /Fatima Memorial Hospital, Shadman, Lahore (Pakistan).
Correspondence: Dr. Muhammad Amjad Khan, Associate Professor, Department of Anesthesiology & Intensive Care, FMH College of Medicine & Dentistry /Fatima Memorial Hospital, Shadman, Lahore (Pakistan) ; Phone: +923214041498; E-mail: amjadfmh@hotmail.com
ABSTRACT:
Introduction: Postoperative nausea and vomiting (PONV) occurs in patients during the first 24 hours of the surgery. Many drugs have been used for the prevention and treatment of PONV. In this trial, we used gabapentin to evaluate its prophylactic effect in reducing the severity and incidence of PONV in patients undergoing diagnostic laparoscopic gynecological surgery.
Methodology: This, double blind randomized controlled trial, was done in operation theatre complex over a period of six months.140 patients undergoing diagnostic gynecological laparoscopic surgery were selected. Two groups were formed and 70 patients were recruited in each group using lottery method as method of randomization. Group C (control group) was given placebo medication orally two hours before surgery and Group G (gabapentin group) received 600 mg of gabapentin orally two hours before the procedure. Standard general anesthesia technique was used in all patients and incidence and severity of postoperative nausea and vomiting (PONV) was recorded in these patients till 24 hours of laparoscopy.
Results: Severity of PONV was graded from mild to severe. There was no PONV in 25 patients (35.7%) in Group C and 47 patients (67.1 %) in Group G. It was mild in severity in 8 patients (11.4 %) in Group C and 5 patients (7.1 %) in Group G, moderate in 31 patients (44.3 %) in Group C and 15 patients (21.4 %) in Group G and severe PONV was seen in 6 patients (8.6%) in Group C and 3 patients (4.3 %) in Group G (P=0.003). Postoperative nausea and vomiting within 24 hours after procedure was present in 45 patients (64.3%) in Group C and 23 patients (32.9%) in Group G. Results were significant between two groups after statistical analysis with p value of 0.001.
Conclusion: Administration of 600 mg of gabapentin two hours before diagnostic gynecological laparoscopy decreases the frequency and severity of PONV.
Key words: Postoperative nausea and vomiting; Gabapentin; Diagnostic Gynecological Laparoscopy
Citation: Khan MA, Siddiqi KJ, Khan MS. Prophylactic use of gabapentin to reduce postoperative nausea and vomiting in patients undergoing diagnostic gynecological laparoscopy. Anaesth, Pain & Intensive Care 2017;21(1):19-24
Received: 30 Jan 2017; Reviewed: 9 Mar 2017; Corrected: 12 Mar 2017; Accepted: 20 Mar 2017
INTRODUCTION:
Postoperative nausea and vomiting (PONV) is commonly seen in operated patients in first 24 hours of surgery and anesthesia. It is a complex problem and its rate is increasing in surgical patients.1 Despite the use of better anesthetics and perioperative medications2 and improvement in operative technique,3 there is still an unacceptable frequency of PONV with an incidence up to 85% reported in some studies.4 The incidence is more than 50% after day case gynecological laparoscopy.5 Laparoscopy is considered an important risk factor for PONV. Female gender, use of opioids in perioperative period and history of previous PONV, motion sickness and smoking are also considered important etiological risk factors.6-8 PONV has various adverse effects on outcome of the patients. It can aggravate pain and can result in unplanned hospital admission. It can increase the risk of pulmonary aspiration leading to aspiration pneumonia and recurrent vomiting can cause dehydration and electrolyte imbalance.5 Due to all these hazardous effects, PONV in patients undergoing day case surgeries can cause severe economic problems by delaying their hospital discharge.9
Various strategies are used to reduce the occurrence of PONV. These include use of single or multiple prophylactic antiemetic agents, modifying anesthetic technique or applying all of them in a multimodal approach to achieve maximum protection.4,10
Prophylaxis of PONV means administration of an antiemetic drug before the start of surgery or during the surgery. Commonly used antiemetic drugs are metoclopramide, cyclizine, droperidol, ondansetron and dexamethasone. These drugs decrease the incidence of PONV by 50%.11-15 However, despite use of all these agents, many anesthetists still face this problem in their patients.
Gabapentin, an antiepileptic drug, was introduced in clinical practice in 1993. It is similar in structure to gamma amino butyric acid (GABA).16 Antiemetic effect of gabapentin was indicated by a clinical trial in which it was used for treatment of chemotherapy induced nausea and vomiting in patients of breast cancer.17 In another study, it was used as prophylactic antiemetic in patients undergoing laparoscopic cholecystectomy. This study showed that the incidence of PONV was significantly lower in patients of gabapentin group versus in patients receiving placebo.18
In our study, we hypothesized that prophylactic use of 600 mg of gabapentin two hours before anesthesia would decrease the incidence and severity of PONV in high risk group of patients undergoing elective gynecological laparoscopic surgery.
Primary objective was to determine the efficacy of gabapentin as prophylactic antiemetic to reduce the rate and severity of postoperative nausea and vomiting (PONV) in patients undergoing elective diagnostic laparoscopy for gynecological problems. Secondary objective was to determine the frequency of use of rescue antiemetic (ondansetron) for management of PONV and consumption of opioids for treatment of postoperative pain.
METHODOLOGY:
This randomized double-blind controlled trial was done in operation theatre complex of hospital over a period of almost six months. Approval from institutional review board was obtained and 140 female patients of ASA I & ASA II physical status, aged 20-40 years, scheduled for elective diagnostic gynecological laparoscopy for problems of infertility, chronic pelvic pain and ectopic pregnancy were included in the study. Two groups were formed having 70 patients in each group. Study group was labelled as Group G and control group was labelled as Group C. All patients were explained about the study and consent was obtained from them. The calculated sample size, with 10% margin of error and 80% power of study with magnitude of prevention of PONV by gabapentin in previous studies (i.e. 62.2%) , was 140 patients. The patients having history of cardiovascular diseases, acid peptic disease, epilepsy, renal or hepatic diseases, coagulopathy and patients on antidepressants or calcium channel blockers were excluded from the study. The patients sensitive to any drug and not willing for study were also not included. Lottery method was used as method of randomization to allot 70 patients to each group and a randomization list was generated. The capsules containing gabapentin and placebo were identical and were prepared by the pharmacy. Study group G (70 patients) received 600 mg of gabapentin orally two hours before induction of anesthesia and control group C (70 patients) received capsules containing placebo (starch powder) orally two hours before anesthesia. Patients, researcher and staff nurse in postanesthesia care unit (PACU) were all blinded to treatment groups.
Following were the variables in this study; Ages and weights of the all patients to be recorded in data forms. Following were the dependent variables which were to be recorded by designated staff nurse of PACU till 24 hours of anesthesia. She was blinded of treatment groups.
1- Incidence and severity of PONV was graded as;
Absent = Absence of any episode of nausea or vomiting
Mild = One episode of vomiting with short lasting nausea of less than 10 min and no antiemetic required.
Moderate = 1-2 episodes of vomiting with moderate nausea and one-time antiemetic used for this.
Severe = More than 2 episodes of vomiting with severe nausea and antiemetic used for each episode.
2- Use of rescue antiemetic (ondansetron 0.1 mg/Kg).
3- Use of rescue analgesia for postoperative pain (nalbuphine 0.05 mg/Kg).
Anesthetic technique was standardized for both the groups. Standard general anesthesia was administered to all patients. Induction of anesthesia was achieved with Propofol 2 mg/kg and nalbuphine 0.15 mg/kg intravenously (IV). Atracurium besylate 0.5 mg/kg was given intravenously to achieve muscle relaxation for tracheal intubation. Bag mask ventilation continued for three minutes with 50% oxygen in nitrous oxide and isoflurane 0.6% through closed circuit with fresh gas flow at 6 lit/min. Tracheal intubation was done with 7.5 mm endotracheal tube. 40% oxygen in nitrous oxide, isoflurane 0.6 – 1.0 % and fresh gas flow rate @ 3 liters per minute was used for maintenance of anesthesia. Intermittent boluses of 10 mg of atracurium besylate were given to maintain muscle relaxation. Maintenence and deficit fluid was replaced using Ringer’s lactate according to weight of the patients. When laparoscopic procedure finished and there were two twitches on train of four on nerve stimulator, the patients were reversed with neostigmine 2.5 mg and glycopyrrolate 0.4 mg intravenously. ECG, pulse oximetry, noninvasive blood pressure, end tidal capnography and neuromuscular function monitor were used for monitoring of all patients. Nalbuphine 0.05 mg/kg two hourly was used intravenously for treatment of postoperative pain. Ondansetron 0.1 mg/kg intravenously was used as rescue antiemetic for any episode of PONV within 24 hours of surgery.
In PACU, patients were assessed 4 hourly by the staff nurse who was blinded of groups and information of incidence and severity of PONV (no, mild, moderate & severe) , use of rescue antiemetic and supplemental analgesic requirements were recorded by her in data forms till 24 hours.
Statistical Analysis: At the end of study, all the information collected was entered and processed in SPSS 10.0 for statistical results. The qualitative variables such as postoperative nausea and vomiting and rescue antiemetic use were presented as percentages and frequencies. Quantitative variables such as age, weight and number of times rescue analgesia used were presented as mean and standard deviation. Chi-square test was applied as test of significance and a p-value of < 0.05 was considered significant.
RESULTS:
All 140 patients undergoing diagnostic gynecological laparoscopy completed the study with 100% participation from both groups (Table 1).
Table -1: Distribution of patients according to groups
| *Group | Frequency (n) | Valid Percentage | Cumulative Percentage |
| G | 70 | 100 | 100 |
| C | 70 | 100 | 100 |
| Total | 140 | 100 |
*G= Gabapentin Group, C= Control Group
All the patients were 20 to 40 years of age with means of 28.56 ± 4.15 years in Group C and 28.59 ± 4.18 years in Group G. Weights of patients were from 45 to 77 kg and mean weight was 60.16 ± 7.14 kg in Group C and 57.30 ± 6.7 kg in Group G (Table 2).
Table-2: Demographic data of patients
| Parameter | Group C (Placebo) | Group G(Gabapentin) | ||||
| Minimum Value | Maximum Value | Mean ± SD | Minimum Value | Maximum Value | Mean ± SD | |
| Age (years) | 20 | 40 | 28.56 ± 4.15 | 20 | 40 | 28.59 ± 4.18 |
| Weight(Kg) | 45 | 77 | 60.16 ± 7.14 | 45 | 77 | 57.30 ± 6.7 |
PONV was absent in 25 (35.7%) patients in Group C and 47 (67.1%) patients in Group G. It was mild in severity in 8 (11.4%) patients in Group C and 5 (7.1%) patients in Group G. Moderate PONV was observed in 31 (44.3%) patients in Group C and 15 (21.4%) patients in Group G. It was severe in 6 (8.6%) patients in Group C and 3 (4.3%) patients in Group G. Results were significant as p value was 0.003 (Table 3).
The rescue antiemetic (ondansetron) was used in 37 (52.9%) patients in Group C and 17 (24.3%) patients in Group G. So results were statistically analyzed and found significant with p value of 0.001 (Table 4).
Table-3: Distribution of cases by severity of PONV
| Grade of Severity | Group C (Placebo)
n (%) |
Group G (Gabapentin)
n (%) |
Statistical analysis
|
| No | 25 (35.7) | 47 (67.1) | Chi Square = 13.980, df = 3 , P value = 0.003 |
| Mild | 08 (11.4) | 05 (7.1) | |
| Moderate | 31 (44.3) | 15 (21.4) | |
| Severe | 06 (8.6) | 03 (4.3) |
Table-4: Use of rescue antiemetic, PONV within 24 hours and Rescue analgesia used
| Variables | Group C
n (%) |
Group G
n (%) |
Chi- Square | P Value |
| Rescue Antiemetic used | 37 (52.9) | 17 (24.3) | 12.05 | 0.001 |
| PONV within 24 hours | 45 (64.3) | 23 (32.9) | 13.84 | 0.001 |
| Times rescue analgesia used
1-2 Times |
15 (21.4) | 63 (90) | 66.70 | ≤ 0.001 |
| 3-4 Times | 55 (78.6) | 07 (10) |
Postoperative nausea and vomiting within 24 hours was present in 45 (64.3%) patients in Group C and 23 (32.9%) patients in Group G with p value of 0.001 (Table 4).
Rescue analgesia was used 1-2 times in 15 (21.4%) patients in Group C and 63 (90%) patients in Group G. In Group C, rescue analgesia was used 3-4 times in 55 (78.6%) patients. While 7 (10%) patients in Group G received rescue analgesia 3-4 times. So results were significant with p value of 0.001 (Table 4).
DISCUSSION:
Laparoscopic surgery is commonly performed, especially for diagnostic purposes in gynecological patients. Most of these gynecological laparoscopic procedures are done routinely on day case basis and are short in duration. However, certain postoperative problems like nausea & vomiting and pain can delay the discharge of these day case patients from the hospital. The trials have proved that postoperative nausea and vomiting (PONV) is common after anesthesia and surgery and its overall incidence is from 28-30%.19
Our study also showed a lower incidence and severity of postoperative nausea and vomiting in diagnostic laparoscopy in gynecological patients who received 600 mg of gabapentin two hours before anesthesia than those who received placebo (32.9% vs 64.3%).
Causes of postoperative nausea and vomiting after gynecological laparoscopy are not clear but might be associated with operative factors. The most important factor is intraperitoneal CO2 insufflation which causes peritoneal stretching and irritation.20 Other factors having affect on PONV are age, female gender, obesity, technique of anesthesia, presence of pain, use of opioid for pain management and type and duration of surgery.21 In our study, the duration of surgery was also short which might decrease the incidence of PONV and mean ages were 28.56±4.15 in Group C and 28.59±4.18 in group which indicated that our patients were from high risk group as incidence of PONV is maximum in this young age group. Apfil et al demonstrated in a study that female gender, previous history of motion sickness & PONV, smoking and use of opioids for treatment of postoperative pain increased the incidence of PONV by 10-21%, 39%, 61% and 79% respectively.22
In our study all patients were nonsmokers and there was no history of motion sickness and there was no gender difference. So both groups were comparable regarding this.
In a trial, Guttuso et al used gabapentin as antiemetic for treatment of acute and delayed onset nausea and vomiting induced by chemotherapy. They used oral 300 mg of gabapentin twice daily in nine patients who were receiving chemotherapy for breast cancer. Six patients showed great improvement on incidence of nausea and vomiting while there was complete resolution in three patients.16
Pandey et al conducted a randomized control trial in which 600 mg of gabapentin was used two hours before anesthesia for prevention of postoperative nausea and vomiting in patients undergoing for laparoscopic cholecystectomy. It was seen that patients of gabapentin group had quite lower incidence of PONV within 24 hours than placebo group (37.8% vs 64%).17. Our study also showed similar results with decrease in incidence of PONV within 24 hours in gabapentin group as compared to placebo group (32.9% vs 64.3%) but we used same dose of gabapentin in young female patients of diagnostic gynecological laparoscopy who were high risk group for PONV. This fact further encouraged its use in day case young patients because effective control of PONV would help in timely discharge of these patients from the hospital.
Apart from its antiemetic effect, different studies have shown that gabapentin reduced the pain scores and opioids requirements in surgically operated patients.23,24 Our study also showed that opioids requirements were quite less in gabapentin group as compared to control group. As use of opioids for postoperative pain is an important risk factor for PONV, so less opioid use in gabapentin group might also decrease the occurrence and severity of PONV in these patients. Our study also showed that there was no discernible effect on somnolence in gabapentin group. So due to all these reasons, it can be used safely in day case young patients.
CONCLUSION:
Prophylactic use of 600 mg of gabapentin two hours before diagnostic gynecological laparoscopy decreases the incidence and severity of postoperative nausea and vomiting and it also decreases the opioids requirements. Therefore, gabapentin can be given preoperatively for its antiemetic and analgesic effects as it was well tolerated by all patients in this study.
REFERENCES:
1- Shaikh SI, Nagarekha D, Hegade G, Marutheesh M. Postoperative nausea and vomiting: A simple yet complex problem. Anesth Essays Res. 2016 Sep-Dec;10(3):388-396. [PubMed] [Free full text]
2- Won YJ, Yoo JY, Chae YJ, Kim DH, Park SK, Cho HB et al. The incidence of postoperative nausea and vomiting after thyroidectomy using three anaesthetic techniques. J Int Med Res. 2011;39(5):1834-42. [PubMed]
3-Yoo JY, Chae YJ, Cho HB, Park KH, Kim JS, Lee SY. Comparison of the incidence of postoperative nausea and vomiting between women undergoing open or robot-assisted thyroidectomy.Surg Endosc. 2013 Apr;27(4):1321-5. doi: 10.1007/s00464-012-2607-7 [PubMed]
4- Gan TJ, Diemunsch P, Habib AS, Kovac A, Kranke P, Meyer TA et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2003 Jul;97(1):62-71. [PubMed]
5- Rusch D, Palm S, Sauerwald M, Romer T, Wulf H. Prophylaxis of postoperative nausea and vomiting following gynecological laparoscopy. Anaesthesiol Intensivmed Notfallmed Schmerzther 2002 Jan; 37(1): 16 – 23 [Free full text]
6- Miller RD, Pardo MC, eds. Basics Of Anesthesia. 6th ed. Philadelphia: Elsevier & Saunders; 2011:642-643.
7- Habib AS, White WD, Eubanks S, Pappas TN, Gan TJ. A randomized comparison of a multimodal management strategy versus combination antiemetics for the prevention of postoperative nausea and vomiting. Anesth Analg. 2004 Jul;99(1):77-81. [PubMed]
8- Bel Marcoval I, Gambús Cerrillo P. [Risk assessment, prophylaxis and treatment for postoperative nausea and vomiting]. Rev Esp Anestesiol Reanim. 2006 May;53(5):301-11. [PubMed]
9- Odin I, Merle JC, Feiss P, Nathan N.[ Postoperative nausea and vomiting: Cost and therapeutic algorithm. Part II; high risk patients and late PONV] Ann Fr Anesth Reanim. 2004 Jun;23(6):581-588. [PubMed]
10- Chandrakantan A, Glass PS. Multimodal therapies for postoperative nausea and vomiting, and pain. Br J Anaesth. 2011 Dec;107 Suppl 1:i27-40. [PubMed] [Free full text]
11-Yuksek MS, Alici HA, Erdem AF, Cesur M. Comparison of prophylactic anti-emetic effects of ondansetron and dexamethasone in women undergoing day-case gynaecological laparoscopic surgery. J Int Med Res. 2003 Nov-Dec;31(6):481-8. [PubMed]
12- Johns RA, Hanousek J, Montgomery JE. A comparison of cyclizine and granisetron alone and in combination for the prevention of postoperative nausea and vomiting. Anaesthesia. 2006 Nov;61(11):1053-7. [PubMed] [Free full text]
13-Laiq N, Khan MN, Qureshi FA, Khan S, Jan AS. Dexamethasone as antiemetic during gynaecological laparoscopic surgery.J Coll Physicians Surg Pak. 2005 Dec;15(12):778-81. [PubMed]
14- Jamil M, Gilani SM, Khan SA. Comparison of metoclopramide prochlorperazine and placebo in prevention of PONV following tonsillectomy in young adults. J Ayub Med Coll Abbottabad. 2005 Oct-Dec;17(4):40-4. [PubMed]
15- Nesek-Adam V, Grizelj-Stojcić E, Mrsić V, Smiljanić A, Rasić Z, Cala Z. Prophylactic antiemetics for laparoscopic cholecystectomy: droperidol, metoclopramide, and droperidol plus metoclopramide. J Laparoendosc Adv Surg Tech A. 2004 Aug; 14(4):212-8. [PubMed]
16- Kunihara M, Sase S, Arakawa A. [A novel antiepileptic, gabapentin (GABAPEN)]. Nihon Yakurigaku Zasshi. 2007 Apr;129(4):299-307. [PubMed]
17- Guttuso T Jr, Roscoe J, Griggs J. Effect of gabapentin on nausea induced by chemotherapy in patients with breast cancer. Lancet. 2003 May 17;361(9370):1703-5. [PubMed]
18- Pandey CK, Priye S, Ambesh SP, Singh S, Singh U, Singh PK. Prophylactic gabapentin for prevention of postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy: a randomized, double-blind, placebo-controlled study. J Postgrad Med. 2006 Apr-Jun;52(2):97-100. [PubMed] [Free full text]
19- Cohen MM, Duncan PG, DeBoer DP, Tweed WA.The postoperative interview: assessing risk factors for nausea and vomiting.Anesth Analg. 1994 Jan;78(1):7-16. [PubMed]
20- Haigh CG, Kaplan LA, Durham JM, Dupeyron JP, Harmer M, Kenny GN. Nausea and vomiting after gynaecological surgery: a meta-analysis of factors affecting their incidence. Br J Anaesth. 1993 Oct;71(4):517-22. [PubMed]
21- Sinclair DR, Chung F, Mezel G. Can postoperative nausea and vomiting be predicted. Anesthesiology. 1999 Jul;91(1):109-18 [PubMed] [Free full text]
22- Apfel CC, Laara E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting:conclusions from cross validations between two centers. Anesthesiology. 1999 Sep;91(3):693-700. [PubMed] [Free full text]
23-Pandey CK, Priye S, Singh S, Singh U, Singh RB, Singh PK. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anaesth. 2004 Apr;51(4):358-63. [PubMed]
24-Rorarius MG, Mennander S, Suominen P, Rintala S, Puura A, Pirhonen R, et al. Gabapentin for the prevention of postoperative pain after vaginal hysterectomy. Pain. 2004 Jul;110(1-2):175-81. [PubMed]
↧
A randomized, double blind study comparing fentanyl with ketamine for transient chest discomfort/pain during LSCS under spinal anesthesia
Yashpal Singh, MD1, Shashi Prakash, MD1, Neeraj Kumar, MD2, Atul Kumar Singh , MD1, Bikram Kumar Gupta, MD1, Ram Badan Singh, MD3
1Assistant Professor; 2Senior Resident; 3Professor
Department of Anesthesiology, Institute of Medical Sciences, BHU, Varanasi-221005, UP, India
Correspondence: Dr. Yashpal Singh, Assistant Professor, Department of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, UP, (India); Phone: 91-9918424416; E-mail: dryashacin1999@rediffmail.com
ABSTRACT:
Objective: Intraoperative transient chest discomfort/pain is a common problem during lower segment cesarean section (LSCS), incidence ranging from 30-60 %. Only a few drugs are available to treat it due to concerns regarding maternal and fetal safety. Fentanyl is commonly used but has limited or no availability in most of India especially in rural areas. So we planned this study to compare ketamine as alternative to fentanyl to treat this chest discomfort/pain.
Methodology: This prospective, randomized, double blind study was carried out on sixty patients aged above 18 years, of American Society of Anesthesiologist (ASA) grade I or II scheduled for elective LSCS under spinal anesthesia, who complained of chest discomfort/pain within 15 min of delivery of baby. The parturients were randomly divided into two groups. Group F to receive inj fentanyl 1 µg/kg and Group K to receive inj ketamine 0.25 mg/kg intravenously immediately after complaining of chest discomfort/pain. Duration of surgery, time of onset of pain, time required to relieve pain, hemodynamic parameters, adverse event and duration of postoperative analgesia were observed. The drugs were compared by using equivalence test; Two-One-Sided-Test (TOST).
Results: There was no difference in demographic profile and baseline parameter in both groups. After drug administration chest discomfort/pain was relieved in both groups effectively in 1.15 ± 0.83 min vs. 1.23 ± 0.48 min in Group F and Group K respectively, without any significant adverse event.
Conclusion: Low dose ketamine can be used as alternative to fentanyl for transient retrosternal chest discomfort/pain during LSCS.
Key words: Retrosternal chest discomfort; Fentanyl; Ketamine
Citation: Singh Y, Prakash S, Kumar N, Singh AK, Gupta BK, Singh RB. A randomized, double blind study comparing fentanyl with ketamine for transient chest discomfort/pain during LSCS under spinal anesthesia. Anaesth, Pain & Intensive Care 2017;21(1):73-78
Received: 10 Jul 2016; Reviewed: 4, 11, 14, 20 Sep 2016, 11 Apr 2017; Corrected: 8, 13 Sep 2016, 11, 12 April 2017; Accepted: 12 April 2017
INTRODUCTION :
It has been observed that pain that occurs during lower segment cesarean section (LSCS) under spinal anesthesia have different etiology and occur at various stages of LSCS. Pain during LSCS can occur at the following points; 1- skin incision, this indicates an extremely poor level of regional anesthesia; 2 – peritoneal incision, this occurs prior to the uterine incision; exteriorization of the uterus; 3 – traction on the uterosacral ligaments or bladder; 4 – swabbing of the paracolic gutters; 5 – shoulder tip pain, this may be related to blood or amniotic fluid irritating the diaphragm (referred pain from the phrenic nerve, C3-C5); and 6 – chest pain, rarely this may be accompanied by ECG changes.1,2 The cause of chest discomfort/pain is unknown although small venous air emboli or coronary artery/ esophageal spasm/reflux have been suggested. Chest discomfort/pain usually occurs immediately after delivery of baby. The treatment options are limited, intravenous fentanyl /alfentanil /tramadol/ketamine or a 50:50 mixture of oxygen and nitrous oxide (Entonox) or 0.8% sevoflurane by anesthesia machine.3,4
Acute pain consists of basal or background pain with spikes of more intense pain layered on top of this background. The basal or background pain that can fluctuate over time is called breakthrough pain.5 Breakthrough pain, related to some specific activity is known as incidental pain. There is no literature addressing treatment of incidental pain occurring on operating table immediately after cesarean section. Intravenous opioids are well studied for intra-operative or postoperative pain relief but limited availability of short acting opioids like fentanyl or alfentanil, especially in rural/remote areas of developing countries prevents their use. Ketamine is well known and popular in every place, including rural areas. There is paucity of literature to treat this type of pain. So we planned this study to compare ketamine as an alternative to fentanyl for effectiveness to relieve chest discomfort/pain during LSCS.
METHODOLOGY:
After approval from hospital ethical committee, and informed consent, 60 patients aged above 18 years, of American Society of Anesthesiologist (ASA) grade I or II scheduled for elective LSCS under spinal anesthesia, and who complained of intra-operative chest discomfort/pain were included in this prospective, randomized-controlled, double-blinded trial. Patients with history of hypertension, ischemic heart disease, rheumatic heart disease, reflux esophagitis, disarranged hepatic or renal function, head trauma, psychiatric diseases, and sensitivity to studied drugs or contraindication to spinal anesthesia were excluded from the study.
All patients were randomly assigned to two equal groups. Randomization was done by an investigator involved in drug administration and data collection. Concealment was done via the sealed opaque envelope technique. Data analysis was carried out by another investigator blinded to group allocation. Patients complaining of chest discomfort/pain within 15 min after delivery of baby were included in the study. Group F to receive inj fentanyl 1 µg/kg and Group K to receive inj ketamine 0.25 mg/kg IV immediately after complaining of chest discomfort/pain. Duration of surgery, time of onset of pain, time required to relieve pain, hemodynamic parameters, adverse events were observed.
Premedication included tab ranitidine (150 mg), and tab metoclopramide (10 mg) administered orally on the evening before surgery and 2 h before the scheduled procedure. On arrival to the operative room, monitors were placed and baseline parameters recorded. All patients were preloaded with lactated ringer solution (15 ml/kg) via 18 G peripheral
IV catheter. Before the commencement of spinal anesthesia, patients were explained about the chest discomfort/pain. In the lateral decubitus position under standard aseptic precautions, using a midline approach lumbar puncture was performed at L3-L4 or L4-L5 intervertebral space by 25 gauge Quincke spinal needle (BD, Gurgaon, Haryana, India). Having confirmed the free flow of cerebrospinal fluid through the spinal needle, Bupivacaine (heavy) 2.5 ml solution was injected intrathecally over a period of 10–15 sec. and patients were turned to the supine position. Surgery was not allowed till bilateral sensory block reaches up to T4 level. Just after delivery of baby all patients received oxytocin 5 units slow IV over 2-3 min and 10 units in 500 ml of dextrose normal saline slow infusion over 3-4 hours according to protocol. Any episode of hypotension (systolic blood pressure < 90 mmHg or > 25% below baseline) was managed by ephedrine (5 mg) and an additional fluid bolus of ringer lactate solution. Bradycardia (< 50 beats/min) was managed by inj atropine 0.5 mg IV bolus.
Statistical analysis: The statistical analysis was performed with Minitab 17 statistical software by using Two One-Sided Test (TOST) for equivalence, for comparison of hemodynamic parameters and time required to relieve chest discomfort. In this study we wanted to prove that ketamine could be safely used in place of fentanyl, and was not significantly inferior to fentanyl; thus it was a non-inferiority study. TOST is the appropriate test for this study which can prove that two means are sufficiently equivalent (Figure 1).
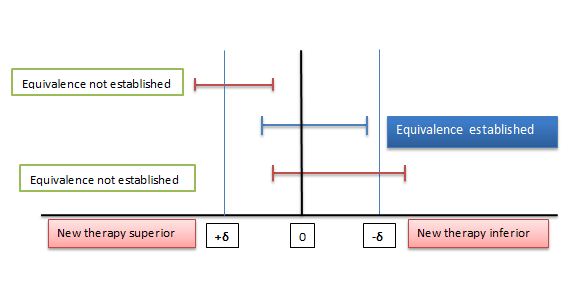
Figure 1: Two One-Sided Test procedures (TOST) and the equivalence margin in equivalence testing. δ: Equivalence margin
The equivalence margin, denoted by δ is the important feature of equivalence or non-inferiority test. Equivalence margin of difference is set as 20% of mean value. If 90% confidence interval is within the equivalence interval, we can claim equivalence. If greater of the two p-values is < 0.05 then we claim that two means are same
RESULTS:
All 60 patients completed the study successfully (Figure 2). The study groups were comparable in terms of demographic profile, baseline hemodynamic variables, ASA status and the duration of surgery (Table 1).
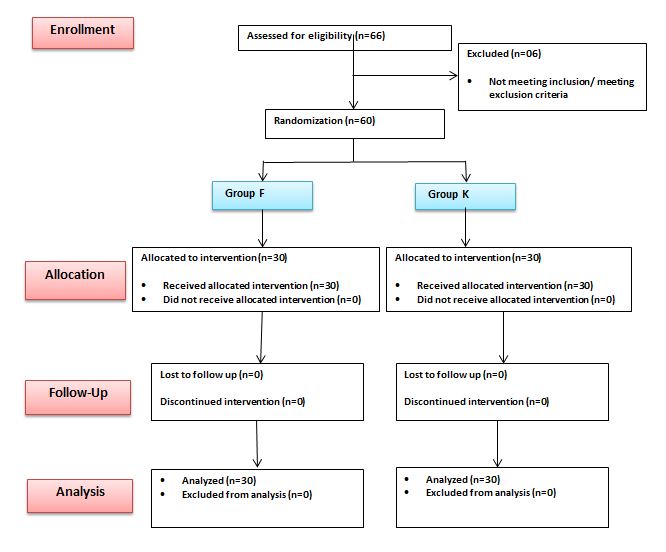
Figure 2: Flow chart of patients studied
Table 1: Demographic profile and baseline parameter between two groups.
| Parameter | Group F | Group K | p value |
| Age (year) | 31.24 ± 3.12 | 30.16 ± 2.32 | 0.134 |
| Body weight(kg) | 53.30 ± 7.07 | 53.35 ± 10.0 | 0.982 |
| Parity | 1.77 ± 0.78 | 1.84 ± 0.94 | 0.754 |
| No. of Previous LSCS | 1.87 ± 0.83 | 1.69 ± 0.56 | 0.329 |
| Duration of surgery(min) | 66.50 ± 16.8 | 66.25 ± 14.94 | 0.951 |
| ASA I/II | 13/17 | 12/18 | 1.00 |
| Baseline heart rate (beats/min) | 92.80 ± 8.65 | 94.12 ± 7.34 | 0.526 |
| Baseline systolic blood pressure (mmHg) | 128.16 ± 10.84 | 127.20 ± 11.13 | 0.736 |
| Baseline diastolic blood pressure (mmHg) | 83.33 ± 12.21 | 84.63 ± 11.39 | 0.641 |
Data are presented as mean ± SD. p value <0.05 considered as significant. LSCS= Lower segment cesarean section, ASA= American Society of Anesthesiologist, SD=Standard deviation
Maximum number of patients developed chest discomfort/pain after administration of oxytocin (about 50%) in both groups followed by time between peritoneal incision and delivery of baby (Table 2).
Table 2: Timing of Retrosternal chest discomfort/pain.
| Timing of Pain | Group F | Group K |
| At peritoneal incision (PI) | 03 (10%) | 02 (6.67%) |
| Between PI and delivery of baby (DB) | 05 (16.67%) | 07 (23.33%) |
| Within 5 min of oxytocin administration | 16 (53.33%) | 14 (46.67%) |
| After 5 min of oxytocin administration | 05 (16.67%) | 06 (20%) |
| At time of peritoneal closure | 01 (3.33%) | 01 (3.33%) |
Data are presented as occurrences or percentage.
After intravenous injection chest discomfort/pain was relieved in 1.15 ± 0.83 min in Group F, while in 1.23 ± 0.48 min in Group K. TOST analysis shows that two means are not equal (Table 3), but this difference 0.08 min (4.8 second) between two groups was not clinically significant.
Table 3: Time required relieving chest discomfort/pain after drug administration
| Parameter | Group F | Group K | Equivalence interval | 90% confidence interval | p value |
| Time (minutes) | 1.15 ± 0.83 | 1.23 ± 0.48 | ± 0.23 | -0.21 0.37 | 0.04 0.19 |
Data are presented as Mean ± SD. SD=Standard deviation. Confidence interval is the outside the equivalence interval and greater of two p value is 0.19, so two means are not equivalent.
There was significant fall in heart rate and systolic blood pressure from baseline value after subarachnoid block in both groups but intergroup comparison shows that two means are equal (Table 4). At onset of chest discomfort/pain, there were transient increase in heart rate and blood pressure from baseline value in both groups but intergroup comparison shows that means are equal (Table 4). After intravenous fentanyl, heart rate and mean arterial blood pressure approaches towards baseline but in ketamine group, heart rate and mean arterial blood pressure remain higher but two means are equal and statistically comparable (Table 5).
Table 4: Systolic blood pressure at different time intervals.
| Systolic blood pressure | Group F | Group K | Equivalence interval | 90% confidence interval | p-value |
| Baseline | 122.16 ± 10.84 | 121.20 ± 11.13 | ± 24.43 | -5.70 3.78 | 0.00 0.00 |
| 5 min after subarachnoid block | 103.27 ± 8.83 | 102.12 ± 8.12 | ± 20.65 | -4.81 2.51 | 0.00 0.00 |
| At onset of chest discomfort/pain | 128.31 ± 9.45 | 127.81 ± 10.13 | ± 25.66 | -4.73 3.73 | 0.00 0.00 |
| 5 min after drug administration | 118.26 ± 9.12 | 130.45 ± 8.98 | ± 23.65 | 8.82 16.09 | 0.00 0.00 |
| 10 min after drug administration | 114.45 ± 8.86 | 125.12 ± 9.24 | ± 22.89 | 6.76 14.58 | 0.00 0.00 |
| 15min after drug administration | 116.37 ± 7.98 | 120.23 ± 8.54 | ± 23.27 | 0.29 7.43 | 0.00 0.00 |
| Postoperative recovery room | 117.68 ± 10.12 | 118.65 ± 9.87 | ± 23.54 | -3.34 5.28 | 0.00 0.00 |
Data are presented as mean ± SD. SD=Standard deviation. Confidence interval is the within the equivalence margin, so two means are equal.
Table 5: Mean Heart rate (per minute) at different time intervals and their comparison with baseline.
| Time Interval | Group F | Group K | Equivalence interval | 90% confidence interval | p value |
| Baseline | 92.80 ± 8.65 | 94.12 ± 7.34 | ± 18.56 | -2.14 4.78 | 0.00 0.00 |
| 5 min after subarachnoid block | 79.60 ± 9.69 | 82.15 ± 8.65 | ± 15.92 | -1.41 6.51 | 0.00 0.00 |
| At onset of chest discomfort/pain | 104.23 ± 8.23 | 106.34 ± 8.45 | ± 20.84 | -1.49 5.71 | 0.00 0.00 |
| 5 min after drug administration | 111.30 ± 8.22 | 118.62 ± 10.24 | ± 22.26 | 3.31 11.33 | 0.00 0.00 |
| 10 min after drug administration | 96.64 ± 8.24 | 99.46 ± 9.34 | ± 19.33 | -0.98 6.62 | 0.00 0.00 |
| 15 min after drug administration | 95.12 ± 7.35 | 96.12 ± 8.42 | ± 19.02 | -2.41 4.41 | 0.00 0.00 |
| Postoperative recovery room | 94.34 ± 6.26 | 96.58 ± 8.11 | ± 18.87 | -0.89 5.37 | 0.00 0,00 |
Data are presented as mean ± SD. SD=Standard deviation. Confidence interval is the within the equivalence margin, so two means are equal.
Adverse events e.g. hypotension, bradycardia were more common in fentanyl group while tachycardia, ECG changes and nausea/vomiting were more common in ketamine group, but the difference was statistically insignificant between two groups (Table 6).
Table 6: Side Effects
| Parameter | Group F | Group K |
| Hypotension | 6 (20) | 4 (13.33) |
| Bradycardia | 3 (10) | 1 (3.33) |
| Tachycardia | 2 (2.67) | 4 (13.33) |
| ECG changes | 8 (26.67) | 9(30) |
| Shivering | 3 (10) | 2 (2.76) |
| Nausea/Vomiting | 2 (2.67) | 4 (13.33) |
Data are presented as occurrences (percentage)
DISCUSSION:
Our study demonstrates that low dose ketamine can be used safely as alternative to fentanyl for relief of transient retrosternal chest discomfort/pain during LSCS.
We selected ketamine because of its easy availability in developing countries, short duration of action and proven analgesic effect at sub-anesthetic dose by various mechanisms.6-9 In gynecologic surgery, there are some studies which used ketamine in sub anesthetic dosage. Sen et al. reported that women who received ketamine (0.15 mg/kg) during spinal anesthesia for LSCS operation had declined diclofenac recruitment in the first day postoperatively.10 Kwok et al. in laparoscopic gynecologic surgery reported that reduced requirement to paracetamol in the first week postoperatively in women who received ketamine (0.15 mg/kg).11
There is significant association between oxytocin administration and chest discomfort; approximately 50% of patients develop chest discomfort within five minute of oxytocin administration. Oxytocin is routinely given after delivery of baby to initiate uterine contraction and to prevent excessive bleeding. It is a vasoactive peptide and receptors are located in uterus, heart and large vessels and produces intense vasoconstrictive effect on uterine, umbilical and coronary artery.12,13 It decreases systemic vascular resistance leads to hypotension and reflux tachycardia.14,15 Mismatch between oxygen supply and demand occurs due to combination of tachycardia, hypotension and coronary vasoconstriction that leads to myocardial ischemia and chest discomfort/pain.16,17 Rest of patients develop chest discomfort/pain may be due to traction on peritoneum, reflux esophagitis, amniotic fluid embolism or small venous micro embolism etc.
Chest discomfort/pain was relieved within two minutes of IV injection of fentanyl or ketamine although the two means are not equal but difference of 4.8 second are not clinically significant. Ketamine causes sympathetic stimulation that lead to increase in heart rate and blood pressure while fentanyl causes decrease in heart rate and blood pressure but statistically not significant and two means are equal.
Women in our study had no considerable side effects and ketamine was tolerated well. Ketamine had some side effects such as urine suppression, hallucination, nausea and vomiting in women.18 Similar to our study, Meer et al. reported that ketamine in anesthesia for cesarean section had lower side effects.19
LIMITATION:
Our study has three main limitations. First, patients and surgeon satisfaction was not checked. Second, we did not access the duration of postoperative analgesia. Third, sample size was small. These results may vary from investigations performed on other ethnic groups due to variations in pain or drug sensitivity.
CONCLUSION:
We conclude that low dose ketamine can be used as a good alternative to fentanyl for relief of transient intra-operative chest discomfort/pain during LSCS under spinal analgesia, without any significant adverse events.
Acknowledgement: We would like to thanks to all technical staff, without whom the study could not have been completed.
Conflict of Interest: None
Author contribution: All authors contributed in the conduct of study, literature search, data analysis and manuscript preparation and review.
REFERENCES:
- Moran C, Ni Bhuinneain M, Geary M, Cunningham S, McKenna P, Gardiner J. Myocardial ischaemia in normal patients undergoing elective caesarean section: A peripartum assessment. Anaesthesia 2001; 56:1051-8. [PubMed] [Free full text]
- Zakowski MI, Ramanathan S, Baratta JB, Cziner D, Goldstein MJ, Kronzon I, et al. Electrocardiographic changes during cesarean section: A cause for concern? Anesth Analg 1993; 76:162-7. [PubMed] [Free full text]
- Rosen M. Nitrous oxide for pain relief of labor pain: a systemic review. Am J Obstet Gynecol. 2002 May;186(5 Suppl Nature):S110-26.[PubMed]
- Yeo ST, Holdcroft A, Yentis SM, Stewart A. Analgesia with sevoflurane during labour: i. Determination of the optimum concentration. Br J Anaesth 2007; 98:105-9. [PubMed]
- Svendsen KB, Andersen S, Arnason S, Arnason S, Arner S, Breivik H, et al. Breakthrough pain in malignant and non-malignant diseases: a review of prevalence, characteristics and mechanism. Eur J Pain. 2005; 9:195–206. [PubMed]
- Joselyn AS, Cherian VT, Joel S. Ketamine for labour analgesia. Int J Obstet Anesth. 2010; 19:122–3. doi: 10.1016/j.ijoa.2009.07.004. [PubMed]
- Ganla KN, Deshmukh S, Bhide A, Desai S. Analgesia in labor by intermittent intravenous bolus ketamine. J Obstet Gynaecol. 2000;4:60–2
- Bauchat JR, Low-dose ketamine with multimodal postcesarean delivery analgesia: a randomized controlled trial, Int J Obstet Anesth. 2011; 20:3-9. doi: 10.1016/j.ijoa.2010.10.002. [PubMed]
- Heesen M1, Böhmer J, Brinck EC, Kontinen VK, Klöhr S, Rossaint R, et al. Intravenous ketamine during spinal and general anaesthesia for caesarean section: systematic review and meta-analysis. Acta Anaesthesiol Scand. 2015 Apr;59(4):414-26. doi: 10.1111/aas.12468. [PubMed]
- Sen S, Ozmert G, Aydin ON, Baran N, Caliskan E. The persisting analgesic effect of low-dose intravenous ketamine after spinal anaesthesia for caesarean section. Eur J Anaesthesiol. 2005; 22:518-23. [PubMed] [Free full text]
- Kwok RF, Lim J, Chan MT, Gin T, Chiu WK. Preoperative ketamine improves postoperative analgesia after gynecologic laparoscopic surgery. Anesth Analg. 2004; 98:1044-9. [PubMed]
- Gutkowska J, Jankowski M, Mukaddam-Daher S, McCann SM. Oxytocin is a cardiovascular hormone. Braz J Med Biol Res 2000; 33:625-33. [PubMed]
- Fortner CL, Manley ES Jr, Woodbury RA. Effects of synthetic oxytocin with and without preservatives upon coronary blood flow in the dog. J Pharmacol Exp Ther 1969; 165:258-66. [PubMed] [Free full text]
- Pinder AJ, Dresner M, Calow C, Shorten GD, O’Riordan J, Johnson R. Haemodynamic changes caused by oxytocin during caesarean section under spinal anaesthesia. Int J Obstet Anesth 2002; 11:156-9. [PubMed]
- Langesaeter E, Rosseland LA, Stubhaug A. Hemodynamic effects of oxytocin during cesarean delivery. Int J Gynaecol Obstet 2006; 95:46-7. [PubMed]
- Svanström MC, Biber B, Hanes M, Johansson G, Näslund U, Bålfors EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100:683-9. doi: 10.1093/bja/aen071. [PubMed]
- Chilvers JP, Cooper G, Wilson M. Myocardial ischaemia complicatingan elective Caesarean section. Anaesthesia 2003;58:822-3. [PubMed] [Free full text]
- Subramaniam K, Subramaniam B, Steinbrook RA. Ketamine as adjuvant analgesic to opioids: a quantitative and qualitative systematic review. Anesth Analg. 2004; 99:482-95. [PubMed]
- Meer FM, Downing JW, Coleman AJ. An intravenous method of anaesthesia for Caesarean section. II. Ketamine. Br J Anaesth.1973; 45:191-6. [PubMed]
↧
Amphotericin B induced hypokalemia in a diabetic patient with rhino-orbitocerebral mucormycosis
Rajeev Sharma, MD1, Sushmita Bairagi, MBBS2, Sashmita Das3, Jyotika Kumar2
1Associate Professor; 2Post Graduate Trainee; 3Registrar
Department of Anesthesiology, Lady Hardinge Medical College & Associated Hospitals, New Delhi, (India)
Correspondence: Dr Rajeev Sharma, M.D, Associate Professor, Lady Hardinge Medical College & Associated Hospitals, New Delhi -110001, (India); Phone: +919990587318; E-mail: rajeevkrsharmaji@gmail.com
ABSTRACT:
Rhino-orbito-cerebral mucormycosis is an aggressive and potentially lethal invasive fungal infection. Surgical debridement and amphotericin B remain the mainstay of treatment, however, associated side effects of amphotericin B like nephrotoxicity, hypokalemia, hypertension and arrhythmias need to be addressed. We discuss the anesthetic management of a 47 year old male with uncontrolled diabetes diagnosed with left sinoorbital mucormycosis posted for surgical debridement. The patient received amphotericin B and insulin preoperatively. Nephrotoxicity due to amphotericin B led to hypokalemia in this patient. We also discuss the role of liposomal formulation in preventing hypokalemia and other side effects associated with use of amphotericin.
Key words: Mucormycosis; Hypokalemia; Amphotericin B
Citation: Sharma R, Bairagi S, Das S, Kumar J. Amphotericin B induced hypokalemia in a diabetic patient with rhino-orbitocerebral mucormycosis. Anaesth Pain & Intensive Care 2017;21(1):90-93
Received: 28 Dec 2016; Reviewed & Accepted: 5 Mar 2017
INTRODUCTION:
Rhino-orbito-cerebral mucormycosis is a fulminant, opportunistic fungal infection commonly seen in diabetes.1 The classic presentation is involvement of nasal mucosa with invasion into paranasal sinuses, orbit and the central nervous system.1 Management includes aggressive surgical debridement, systemic antifungal therapy with amphotericin B (AmB) and treating the underlying comorbidities.2 The nephrotoxic side effect of AmB sometimes requires its discontinuation. Lipid formulation of AmB are better tolerated and used mainly in patients who have already altered renal function.3
CASE REPORT:
A 45 years old male farmer weighing 70 kg presented to the ophthalmology department of our hospital with fever since last10 days, nasal stuffiness associated with bleeding since 6 days, pain and protrusion of left eye since 6 days and diplopia with complete loss of vision in left eye since 2 days. A family history of diabetes was found but the patient had never been evaluated for the same. He was diagnosed one month back with hypertension and was taking oral amlodipine 5 mg and olmesartan 40 mg daily.
Ophthalmologic examination revealed proptosis (Figure 1) and complete loss of vision in left eye with loss of pupillary reflex. MRI showed extensive bilateral ethmoid and left maxillary sinusitis (Figure 2 and 3).

Figure 1: Preoperative photograph of patient showing swelling and proptosis of left eye
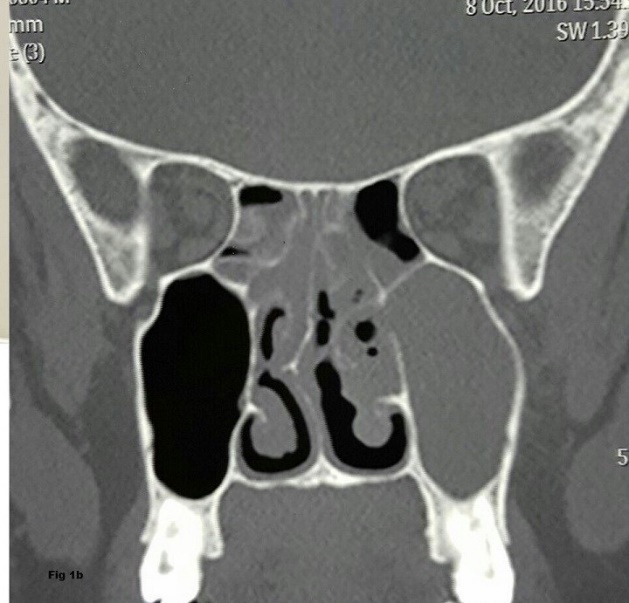
Figure 2: MRI image showing infiltration of maxillary sinus

Figure 3: Infiltration of ethmoid sinus and optic nerve compression
Deviation of nasal septum towards the right side with obliteration of sinus drainage channels was also seen. Frontal and sphenoethmoidal recess was obliterated and left optic nerve compression was reported (Figure 3). Fasting blood sugar was 15.5 mmol/L and HbA1c level was 14.4. He was started on regular subcutaneous insulin which needed to be increased to 18 units per day in three divided doses. The baseline blood urea was 30 mg/dl, serum creatinine was 0.8 mg mg/dl and serum potassium levels (K+) was 4.2 meq/L. Urine sugar was positive but ketones were negative. Otolaryngology consultation was done, nasal swabs were sent for histopathological examination and AmB 1mg/kg/day IV was started along with amoxicillin and clavulanic acid combination 1.2 g 8 hourly. Fungal hyphae were seen on histopathological examination of nasal swabs and a diagnosis of rhino-orbitocerebral mucormycosis was made.
Patient was sent for pre-anesthetic examination for endoscopic surgical debridement after 2 days when the blood sugar charting became normal. Routine investigations were normal except for serum potassium which had decreased to 2.6 meq/L and serum creatinine 1.8 mg/dl. On the day before surgery, AmB was stopped and liposomal inj. AmB 300 mg was started; inj caspofungin 50 mg IV OD and potassium chloride syrup were also added.
On examination, patient was conscious, oriented, responding to verbal commands. Pulse rate was 92/ min, blood pressure was 140/90 mmHg. His fasting blood sugar was 5.5 mmol/l, Na+ – 135 meq/l, K+– 2.6 meq/L, urea-31 mg/dl and serum creatinine – 1.8 mg/dl. Arterial blood gas report showed pH- 7.50, PCO2 – 29.9, PO2 – 106, HCO3 – 23.2. Electrocardiogram and chest x ray were normal.
A written informed consent was taken. Electrocardiogram, noninvasive blood pressure, Pulse Oximeter monitors were attached. Right sided ulnar nerve was used for neuromuscular monitoring using train of four (TOF) ratio. Patient was premedicated with inj. fentanyl 150 micrograms IV and induction was achieved using inj. propofol 140 mg IV. Inj. rocuronium bromide 45 mg was administered after ensuring adequate mask ventilation using oxygen, nitrous oxide and sevoflurane. Orotracheal intubation was performed using a size 8.0 cuffed endotracheal tube on direct laryngoscopy at TOF value of 0. Pharyngeal packing was done around the endotracheal tube.
Anesthesia was maintained using oxygen, nitrous oxide and sevoflurane. Rocuronium was repeated using Train of Four (TOF) ratio. Two IV lines were used for fluid administration. On one side, normal saline infusion was started and on the other side an infusion containing 5% dextrose with 8 unit regular insulin and 20 meq KCl at 100 ml/h was given. Intraoperative blood pressure was in range of 130-140 mmHg systolic and 70-80 mmHg diastolic; blood sugar levels were in range 5.5- 7.7 mmol/L.
Extensive endoscopic surgical debridement was performed in ethmoid and maxillary sinuses and typical mucor infested tissues were removed. Anterior and posterior ethmoidectomy and uncenectomy was done, maxillary osteum was widened and fungal debris was removed. Surgical duration was 90 min. Paracetamol 1 g IV was given for pain relief. On completion of surgery the pharyngeal pack was removed. Inj. ondansetron 8 mg IV was given as antiemetic. Neuromuscular block was reversed with inj. glycopyrrolate 0.6 mg and inj. neostigmine 3.5 mg IV. Tracheal extubation was performed at TOF ratio of 0.9. The patient was monitored in the postoperative unit and later shifted to the ward. Liposomal AmB, insulin and other drugs were continued. The patient showed significant clinical improvement (except for the vision in the left eye which did not improve during hospital stay) his hypokalemia and creatinine gradually improved and was discharged from the hospital after 2 weeks. Consent has been taken from the patient for publication of details.
DISCUSSION:
Rhino orbitocerebral mucormycosis is an opportunistic fungal infection. This fungus thrives in acidic pH and glucose rich medium enhances its growth as it impairs neutrophil chemotaxis and decrease phagocytosis.1,2 This is the reason it is usually seen in diabetic patients. The earliest sign is facial edema, proptosis, chemosis and extraocular muscle paresis, periorbital edema and mucopurulent rhinorrhea.1 Infection spreads rapidly from sinus to orbit to CNS. It occurs by angioinvasion, propagating thrombosis and associated with tissue infarction and necrosis.1 With intracranial extension, MRI is the imaging modality of choice.
Treatment includes extensive surgical debridement, high doses of systemic amphotericin B and control of underlying disease.3 Amphotericin B has its side effects and toxicity that will sometimes requires discontinuation of therapy despite a life-threatening systemic fungal infection.4 Amphotericin B administration causes proinflammatory cytokine production. The acute toxicity includes nausea, vomiting, fever, hypertension or hypotension, and hypoxia.4
Its principal adverse effect is nephrotoxicity. Risk factors of amphotericin B nephrotoxicity include male gender, high average daily dose of amphotericin B (≥ 35 mg/day) diuretic use, body weight ≥ 90kg5, concomitant use of nephrotoxic drugs and abnormal baseline renal function. Clinical manifestation of AmB nephrotoxicity includes renal insufficiency, hypokalemia, hypomagnesemia, metabolic academia and polyuria due to nephrogenic diabetes insipidus.
Our patient was treated with AmB since the day of admission. Liposomal AmB was not available initially and could be added a day before surgery only. The serum K+ level decreased to 2.6 meq/l and Creatinine increased to 1.8 mg/dl which may be due to the nephrotoxic effect of AmB. Studies indicate that renal function is impaired in more than 80% of patients treated with AmB, with 15% of patients requiring hemodialysis.6 The anesthetic management of patients with acute tubular necrosis leading to development of acute renal failure is of particular concern for anesthesia providers. Anesthetic management aims at maintenance of an adequate mean arterial pressure while concomitantly avoiding further renal insults. A heightened awareness for renal, electrolyte, hemodynamic, and respiratory aberrancies is warranted for anesthesia providers when treating patients receiving AmB therapy. AmB induced hypokalemia may enhance the effect of skeletal muscle relaxants when administered concomitantly serum potassium levels should be closely monitored.
Hypokalemia can lead to prolonged duration of action of non depolarising neuromuscular blocking agents and lead to delayed or incomplete recovery after the surgery.7 Hypokalemia also predisposes to arrhythmias and paralytic ileus.7 We used neuromuscular monitoring (TOF) to give optimum doses of rocuronium to avoid these complications.
Since, hypokalemia denotes an intracellular deficit of K+, it important not to aim at its rapid correction in short time period. There were no ECG changes of hypokalemia and we did not aim to correct the levels in the 90 min duration surgery. The patient received oral K+ supplementation preoperatively and low concentration of potassium chloride was given as part of GKI regimen (Glucose-Potassium-Insulin) for diabetes mellitus.
AmB lipid preparations are more tolerable, more efficacious and less nephrotoxic. But due to high cost and relative paucity of clinical data lipid formulations are generally used as second line therapy.
To conclude, we emphasize the importance of adequate blood sugar control, need for urgent surgical debridement, and knowledge about the important side effects of AmB like nephrotoxicity and hypokalemia and its relevance to neuromuscular block and knowledge about the better safety profile of Liposomal AmB in treatment of patients with rhino-orbitocerebral mucormycosis patients.
Conflicts of Interests: None
Financial Disclosures: None
Author contribution: RS: Concept, conduct, writing, editing
SB: Conduct, data
SD: Conduct, data, editing
JK: Conduct, data
REFERENCES:
- Nithyanandam S, Jacob MS, Battu RR, Thomas RK, Correa MA, D’Souza O. Rhino-orbito-cerebral mucormycosis. A retrospective analysis of clinical features and treatment outcomes. Indian J Ophthalmol. 2003 Sep;51(3):231-236. [PubMed] [Free full text]
- Ferguson BJ. Mucormycosis of nose and paranasal sinuses. Otolaryngol Clin North Am. 2000 Apr;33(2):349-65. [PubMed]
- Peterson KL, Wang M, Canalis RF, Abemayor E. Rhinocerebral mucormycosis: evolution of the disease and treatment options. Laryngoscope. 1997 Jul;107(7):855-62. [PubMed]
- Laniado-Laborin R, Cabrales Vargas MN. Amphotericin B: side effects and toxicity. Rev Iberam Mycol. 2009 Dec 31;6(4):223-227. doi: 10.1016/j.riam.2009.06.003. [PubMed]
- Fisher MA, Talbot GH, Maislin G, McKeon BP, Tynan KP, Strom BL. Risk factors for Amphotericin B-associated nephrotoxicity. Am J Med. 1989 Nov;87(5):547–52. [PubMed]
- Wong KC, Schafer PG, Schultz JR. Hypokalemia and anesthetic implications. Anesth Analg. 1993 Dec;77(6):1238-60. [PubMed]
- Walsh TJ, Finberg RW, Arndt C, Hiemenz J, Schwartz G, Bodenstiener D, et al. Liposomal amphotericin b for empirical therapy in patients with persistent fever and neutropenia. National Institute of Allergy and Infectioiou Diseases Mycoses Study Group. N Engl J Med. 1999 Mar;340(10):764–71. [PubMed] [Free full text]
↧